The Affordable Care Act was supposed to make it easier for American workers to switch jobs by making it easier to get health insurance from sources other than their current employer. Mostly it didn’t work out that way. But a new paper finds that one piece of the ACA actually made people less likely to switch jobs.
The ACA Dependent Coverage Mandate required family health insurance plans to cover young adults though age 26, when prior to the 2010 passage of the ACA many had to leave the family plan at age 18 or 19. I thought these newly covered young adults would be more likely to switch jobs or start businesses, but there turned out to be absolutely no effect on job switching, and no overall increase in businesses (though it did seem to increase the number of disabled young adults starting businesses, and other parts of the ACA increased business formation among older adults).
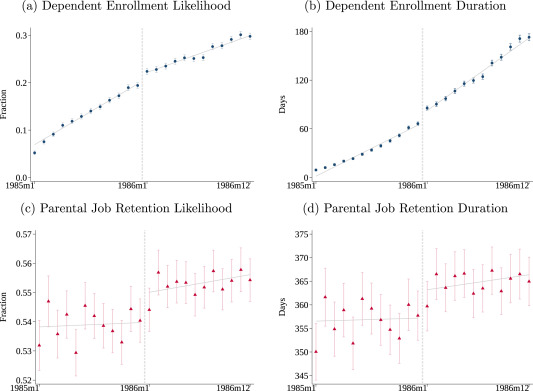
But while the Dependent Coverage mandate seems not to have reduced job lock for young adults, it increased job lock among their parents. That is the finding of a new paper in the Journal of Public Economics by Hannah Bae, Katherine Mackel, and Maggie Shi. Using a large dataset with exact months of age and coverage, MarketScan, allows them to estimate precise effects:
We find that dependents just to the right of the December 1985/January 1986 cutoff—those eligible for longer coverage—are more likely to enroll and remain covered for longer once the mandate is in effect. Dependent enrollment increases by 1.8 percentage points at the cutoff, an increase of 9.2 % over the enrollment rate for dependents born in December 1985. In addition, the enrollment duration increases by 9.7 days (14.6 %). Turning to their parents, we find that parental job retention likelihood increases by 1.0 percentage point (1.8 %) and job duration increases by 5.8 days (1.6 %) to the right of the cutoff. When scaled by the estimated share of dependents on end of year plans, our findings imply that 12 additional months of dependent coverage correspond to a 7.7 % increase in job retention likelihood and a 7.0 % increase in retention duration.
I believe in this parental job lock effect partly because of their data and econometric analysis, and partly through introspection. I plan to work for years after I have the money to retire myself in order to keep benefits for my kids, though personally I’m more interested in tuition remission than health insurance.
On top of working longer though, benefits like these enable employers to pay parents lower money wages. A 2022 Labour Economics paper from Seonghoon Kim and Kanghyock Koh found that the Dependent Coverage Mandate “reduced parents’ annual wages by about $2600 without significant reductions in the probability of employment and working hours.” But at least their kids are better off for it.
Iowa recently joined the growing list of states where midwives or obstetricians can open a freestanding birth center without needing to convince a state board that it is economically necessary. The Des Moines Register provides an excellent summary:
A Des Moines midwife who sued the state for permission to open a new birthing center may have lost a battle in court, but ultimately, she has won the war.
Caitlin Hainley of the Des Moines Midwife Collective sought to open a standalone birthing center in Des Moines, essentially a single-family home repurposed with birthing tubs and other equipment needed to give birth in a comfortable, home-like environment.
To do so, the collective alleged in its 2023 lawsuit, would have required going through a lengthy, expensive regulatory process that would give already established maternity facilities, such as local hospitals, the chance to argue against granting what is known as a certificate of need for the new facility, essentially vetoing competition.
A federal district judge ruled in November that Iowa’s certificate-of-need law is constitutional, finding that legislators had a rational interest in protecting existing hospitals and health care providers.
But while losing the first round in court, the collective’s cause was winning support in a more important venue: the Iowa Capitol. Iowa legislators in their 2025 session passed a bill, which Gov. Kim Reynolds signed on May 1, removing birth centers from the definition of health facilities covered by the certificate-of-need law. The law will formally take effect July 1.
I’m honored to have played a small part in this as the expert witness in the lawsuit.
If you’d like to get involved in making sure birth options are available your state, a great place to start would be to attend the Zoom seminar Roadmap For Reform: Advancing Birth Freedom on July 23rd. It is hosted by the Pacific Legal Foundation, which represented the midwives pro-bono in the Iowa case.
There is strong momentum here with Connecticut, Kentucky, Michigan, Vermont, and West Virginia also recently repealing Certificate of Need requirements for birth centers, but a variety of other barriers remain. States often require freestanding birth centers to obtain a transfer agreement with a nearby hospital before opening to ensure that the hospital will take their emergency cases, even though hospitals are legally required to take all emergency cases. The problem is that hospitals provide both complementary services (emergency care) and substitute services (labor and delivery), and they often choose not to sign transfer agreements in order to prevent competition from a partial substitute. This whole area would benefit both from more academic study, as well as more investigation from antitrust enforcement.
But for today, congratulations to Caitlin Hainley and to Iowa on their victory.
According to the U.S. Department of Agriculture, feral hogs cause approximately $2.5 billion in agricultural damages each year…Nearly 300 native plant and animal species in the U.S. are in rapid decline because of feral swine, and many of the species are already at risk, according to Animal and Plant Health Inspection Service. The swine also carry at least 40 parasites, 30 bacterial and viral illnesses, and can infect humans, livestock and other animals with diseases like brucellosis and tuberculosis.
…They will also feed on tree seeds and seedlings, causing significant damage in forests, groves and plantations… Rooting — digging for foods below the surface of the ground — destabilizes the soil surface, uprooting or weakening native vegetation, damaging lawns and causing erosion. Their wallowing behavior destroys small ponds and stream banks, which may affect water quality. They also prey upon ground-nesting wildlife, including sea turtles. Wild hogs compete for food with other game animals such as deer, turkeys and squirrels, and they may consume the nests and young of many reptiles, ground-nesting birds and mammals.
Pigs are smart (ahead of dogs and horses), tough, and adaptable, and they breed very quickly. The protected, overfed, calm hogs you see on farms quickly turn lean and mean if they have to fend for themselves in the wild. You pretty much only see female pigs or castrated males on the farm, since whole males (boars) are intrinsically aggressive and destructive. But vigorous 200-pound boars, with their 3 inch-long, razor-sharp tusks, are well-represented in feral swine.
This is a growing problem. The population of wild pigs in the southern third of the U.S. has increased significantly in the past few decades. There have historically been some wild pigs in spots like Florida and Texas, escapees from Spanish settlers long ago. But they seem to be spreading northward, largely because hunters transplant them:
From 1982 to 2016, the wild pig population in the United States increased from 2.4 million to an estimated 6.9 million, with 2.6 million estimated to be residing in Texas alone. The population in the United States continues to grow rapidly due to their high reproduction rate, generalist diet, and lack of natural predators. Wild pigs have expanded their range in the United States from 18 States in 1982 to 35 States in 2016. It was recently estimated that the rate of northward range expansion by wild pigs accelerated from approximately 4 miles to 7.8 miles per year from 1982 to 2012 (12). This rapid range expansion can be attributed to an estimated 18-21% annual population growth and an ability to thrive across various environments, however, one of the leading causes is the human-mediated transportation of wild pigs for hunting purposes.
As for pigs attacking and killing humans, a definitive study was recently made in 2023 by Mayer, et al., covering 2000-2019. This report includes informative tables and charts, such as:
and
Comparison of mean annual number of human fatalities from attacks by various wild animals for time periods ranging between 2000 and 2019. From Mayer, et al.
About half of these fatalities occurred in rural regions of India. Government policies there prohibit farmers from killing marauding pigs, so farmers try to chase them away from their fields with rakes and stones. Sometimes that provokes the pig to attack, slashing at thigh level and often lacerating the femoral artery. But a disturbing 39% of deadly attacks were unprovoked, including a horrific case with an elderly woman in Texas. So danger to humans is an issue, though for perspective, far more people are killed each year by snakes (100,000), rabid dogs (30,000), and crocodiles (1000). In the U.S., over 100 people are killed a year, and 30,000 injured, by collisions with deer (see here for a market-based solution for this problem).
What to do? Hunters in many states are free to blast away at feral pigs year-round, since they are considered a harmful, invasive (non-native) species. Paradoxically, however, allowing hunting of pigs can be counterproductive: amateur hunting does not eliminate enough pigs to stop their spread, and it incentivizes hunters to transport pigs to new regions to make for more targets. For instance, Arkansas allows hunting and even transport of pigs, and has seen swine populations skyrocket. The state of Missouri, next door, took the enlightened approach of banning hunting and transport, leaving population control to wildlife professionals. By removing the sport-hunting incentive, Missouri removed the incentive to transport them, which stymied their spread.
To control pig populations, the pros mainly set up baited large corrals, and monitor them remotely with webcams. After several weeks, the local pigs get comfortable coming there to feed. When the cameras show that every single pig in the herd is in the corral, the gate is sprung shut remotely. Then the pros drive out to, er, euthanize the pigs. The goal is to wipe out the entire herd, and leave no sadder-but-wiser survivors who will be harder to catch next time. Once a hog population has become established in an area, it typically takes ongoing eradication efforts to keep the numbers down.
If you want to do your own part to reduce the surplus swine population, the following notable opportunity came to my attention: for a largish fee the Helibacon company will train you in firing automatic weapons and take you up in a chopper where you can mow down a marauding herd in the low Texas scrubland. It sounds like a guy thing, but Helibacon reminds us that full auto is for ladies, too. See also PorkChoppersAviation for similar service.
This is actually a fine example of a free market solution to a problem: wild hogs were such a problem for landowners that they were paying expensive professional helo hunters to take out herds, but in Texas, “All that changed in 2011, when the state legislature passed the so-called pork chopper law, which allowed hunters to pay to shoot feral hogs out of helicopters – and a new business model was born.” Hunters are happy to pay to hunt, helo companies are happy to take their money, and landowners are happy to have pigs reduced for free. Voila, voluntary exchange creates value…
A reporter recently told me she thought there is a national trend toward hospitals issuing more bonds. I tried to verify this and found it surprising hard to do with publicly available data. But once I had to spend an hour digging through private Compustat data to find the answer, I figured I should share some results. Here’s the average debt in millions of companies by sector:
Source: My graph made from Compustat North American Fundamentals Annual data collapsed by Standard Industrial Classification code into the Fama-French 10 sectors
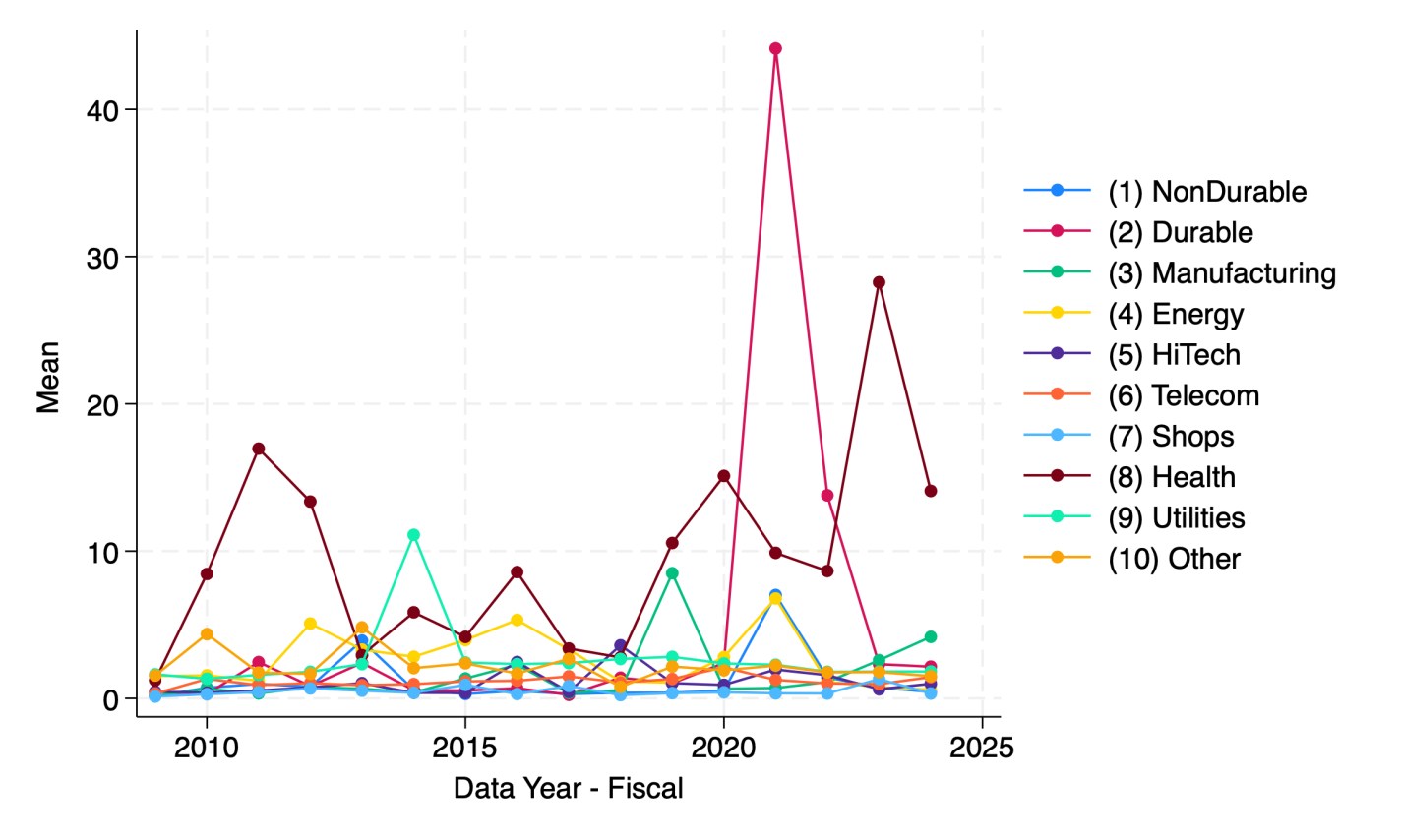
This shows that health care is actually the least-indebted sector, and telecommunications the most indebted, followed by utilities and “other” (a broad category that actually covers most firms in the Fama-French 10). But are health care firms really more conservative about debt, or are they just smaller? Let’s scale the debt by showing it as a share of revenue:
My graph made from Compustat North American Fundamentals Annual data collapsed by SIC code into the Fama-French 10 sectors(dltt/revt).
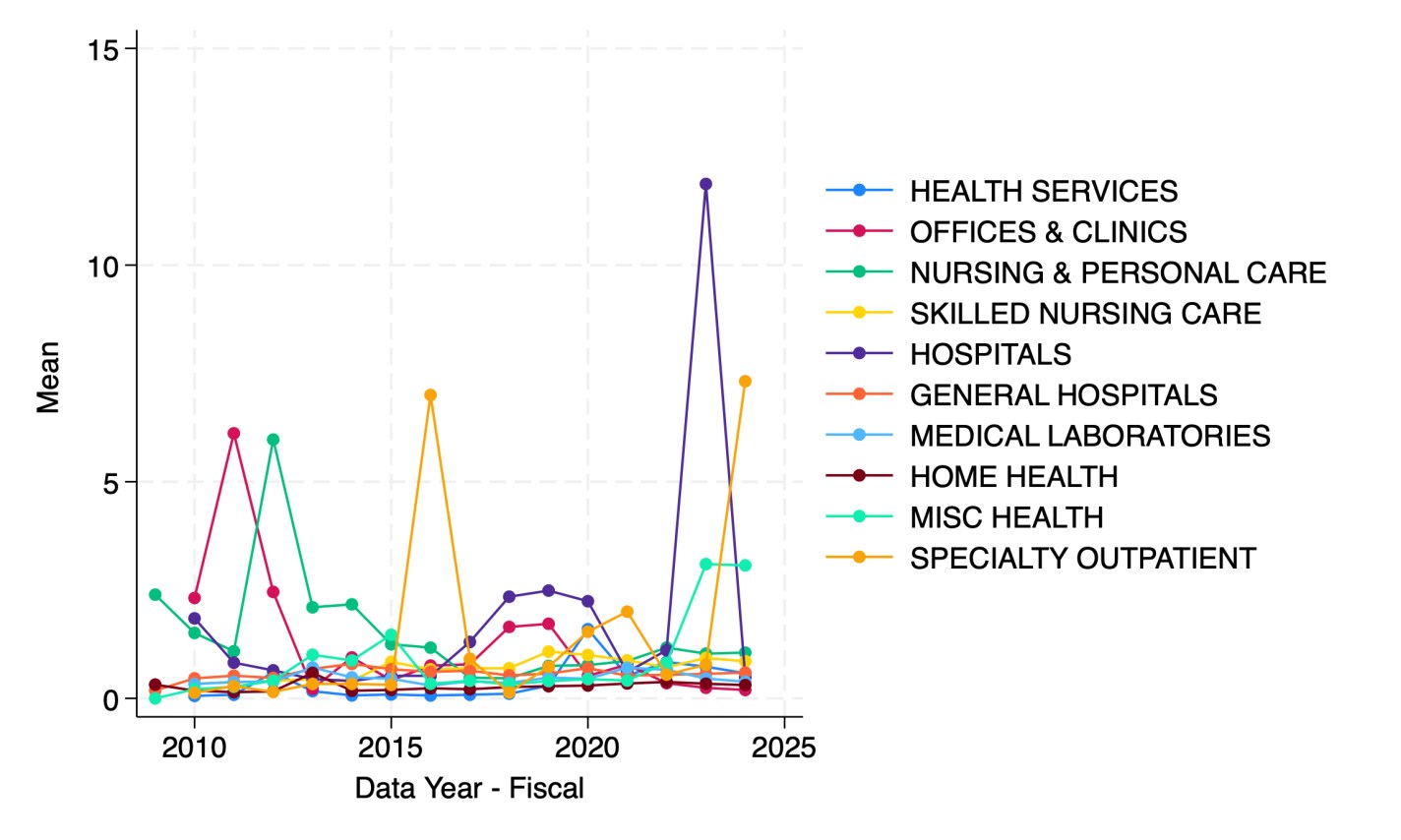
It appears that health care firms are the most indebted relative to revenue since 2023. But which parts of health care are driving this?
Hospitals in 2023 followed by specialty outpatient in 2024. However, seeing how much the numbers bounce around from year to year, I suspect they are driven by small numbers of outlier firms. This could be because Compustat North America data only covers publicly traded firms, but many sectors of health care are dominated by private corporations or non-profits.
I welcome suggestions for datasets on the bond-market side of things that are able to do industry splits including private companies, or suggestions for other breakdowns you’d like to see me do with Compustat.
The United Healthcare Group (UNH) is a gigantic ($260 B market cap, even after recent dip) health plan provider, which until recently seemed to be the bluest of blue-chip companies. It is a purveyor of essential medical services with a wide moat, largely unaffected by tariff posturing, and considered too big to fail. The ten-year stock price chart shows it steadily grinding up and up, shrugging off market tantrums like 2020 and 2022, and even the tragic gunning down of one of its division presidents in December.
But things really unraveled in the past month. Let’s look at the charts, and then get into the underlying causes.
The year-to-date chart above shows the price hanging around $500, then rising to nearly $600 as the April 17 quarterly earnings report approached. Presumably the market was licking its chops in anticipation of the usual UNH earnings beat. The actual report was OK by most corporate standards, but it failed to match expectations. Revenue growth was a hearty +9.8% Y/Y, but this was $2.02B “miss”. Earnings were up 4% over year-ago Q1, but they missed expectation (by a mere 1%). What was probably much more disturbing was guidance on 2025 total adjusted earnings down to $26 to $26.50 per share, compared to $29.74 consensus.
That took the stock down from $600 to around $450 immediately, and then it drifted below $400 in the following month as investors looked for and failed to find better news on the company. But then two things happened last week. The effects are seen in the 1-month chart below:
On May 13 (blue arrow) the company came out with a stunning dual announcement. It noted that the recently-appointed CEO, Andrew Witty, had suddenly resigned “for personal reasons.” The blogosphere speculated (perhaps unfairly) that you don’t suddenly resign from a $25 million/year job unless your “personal reasons” involve things like not going to prison for corporate fraud. The other stunner was that the company completely yanked 2025 financial guidance, due to an unexpected rise in health care costs (i.e., what they must pay out to their participants). Over the next day or two, the stock fell to about 50% of its value in early April.
Then on May 14 the Wall Street Journal came out with an article claiming that the U.S. Department of Justice is carrying out a criminal investigation into UNH for possible Medicare fraud, focusing on the company’s Medicare Advantage business practices. The WSJ said that while the exact nature of the allegations is unclear, it has been an active probe since at least last summer.
UNH promptly fired back a curt response to the “deeply irresponsible” reporting of the WSJ:
We have not been notified by the Department of Justice of the supposed criminal investigation reported, without official attribution, in the Wall Street Journal today.
The WSJ’s reporting is deeply irresponsible, as even it admits that the “exact nature of the potential criminal allegations is unclear.” We stand by the integrity of our Medicare Advantage program.
The stock nose-dived again (red arrow, above), touching 251, as investors completely panicked over “Medicare fraud.” Cooler heads promptly started buying back in, leading to substantial recovery. That includes the new CEO, Steven Hemsley, who was the highly-paid CEO from 2009 to 2017, and since then has been the highly-compensated “executive chairman of the board”, a role created just for him. Pundits were impressed that he stepped in to buy some $25 million of UNH stock near its lows, saying wow, he is really putting some skin in the game. Well, not really: the dude is worth over $1 billion (did I mention high compensation of health care execs?), so $25 mill is hardly heroic. He is already up some 12% or a cool $3 million on this purchase, a tidy little example of how the rich become richer.
The US Department of Health and Human Services has announced it is cutting 10,000 of its 82,000 jobs and restructuring:
As part of the restructuring, the department’s 10 regional offices will be cut to five and its 28 divisions consolidated into 15, including a new Administration for a Healthy America, or AHA, which will combine offices that address addiction, toxic substances and occupational safety into one central office.
AHA will include the Office of the Assistant Secretary for Health, the Health Resources and Services Administration, the Substance Abuse and Mental Health Services Administration, Agency for Toxic Substances and Disease Registry, and the National Institute for Occupational Safety and Health.
These divisions do many different jobs, but as usual what stands out to me is their data- both because it is what I have found directly useful in the past, and because it is what I still have some control over now. Writing your Representatives or writing an op-ed has a minuscule chance of changing Federal policy, but if you download data, you definitely have that data.
What worries me here is that some of the agencies being consolidated might discontinue some of their data products going forward, or even pull some of what they have already created offline. I don’t think this is farfetched given what has happened so far, and given that even in good times these agencies pull down data they painstakingly prepared. For instance, HRSA only publicly posts the State- and County-level Area Health Resources File back to 2019, even though they have annual data going back to 2001.
Probably all 13 of the reorganizing divisions have data worth looking into, and given the staff cuts, even data products in the other divisions could be at risk. But my plan is to focus on the two reorganizing divisions whose data I have previously found useful- HRSA and SAMHSA. HRSA has a nice data download page with 16 different datasets, including the Area Health Resources File, which offers detailed information on the health care workers and facilities in each US county. SAMHSA offers the National Substance Use and Mental Health Services Survey, the Treatment Episode Data Set, and the National Survey of Drug Use and Health. I have previously cleaned and archived the state-level version of the NSDUH, but not the individual-level version that is for now still available from SAMHSA.
All of these datasets are easy to download now, and some will probably become very hard to access later, so now is a good time to take a few minutes and save whatever you think you might need.
Certificate of Need laws require many types of health care providers to obtain the permission of a state board before they are allowed to open or expand in many US states. But there is a lot of variation from state to state in which types of providers are covered by these laws. I put together this map to show the 15 states that require new home health care agencies to obtain a Certificate of Need:
CON states see reduced competition, which tends to be bad news for patients and new entrants, but good for existing providers and the private equity firms consideringbuying them.
But some CON states like Rhode Island have proposed reforms that would exempt home health agencies from the CON process, putting them in line with the majority of states that put new entrants on an even footing with incumbent providers.
A number of weeds growing around your house are edible. Chickweed (Stellaria media) is found in lawns and random areas in cooler climates. It pops out ahead of most other plants in the spring, though it also grows year-round.
It can grow low, hiding in the grass, but it is easier to harvest as a taller standalone clump. Here is a clump from my yard, with the roots and tougher lower parts cut off:
People eat it raw, but I prefer to blanch it first to reduce any bitterness and to get rid of any critters or contaminants. To do that, I got two cups of water boiling in a Pyrex measuring cup, then dropped the chickweed in and stirred it around for a minute, followed by a cool water quench in a colander. The chickweed was then in a wilted state, but still green and crunchy and (as I understand) retaining nearly all its nutrients.
For me, chickweed functions like arugula or cilantro or Italian parsley, as an interesting and worthwhile addition to a salad or sandwich. I would not relish a whole plate of it.
Speaking of nutrients, in folk medicine chickweed is credited with amazing powers. Eat The Planet tells us that:
Chickweed is full of vitamins A, B1, B2, and C as well as fiber and protein. Due to its nutritional contents and numerous medicinal properties, this cold-weather herb has been used in folk medicine for hundreds of years. It can treat many different conditions, such as constipation, bowel problems, iron-deficiency anemia, asthma, bronchitis, joint pains, and blood disorders. It can also aid weight loss by making you feel fuller for longer.
You can also apply the herb directly onto the skin to treat itchiness, bruises, boils, ulcers, and psoriasis. To do this, you can either bruise the leaves or steep the stems in hot water before applying them directly onto the affected areas.
There is no indication that any of the plant’s constituents possess therapeutic activity. Its vitamin content is too low to be of therapeutic value.
Verywellhealth stakes out a middle ground, noting that chickweed has demonstrated significant anti-inflammatory and anti-viral activity in lab experiments with animals, but also noting that these results may or may not translate to efficacy in humans:
Juice or extracts made from chickweed have been studied in test tubes or mice models for the following conditions:
Hepatitis B. Chickweed was shown to have anti-hepatitis B virus activity in a test tube study.
Obesity. Chickweed extract given to overweight mice decreased the amount of food they consumed and their absorption of fats.
Diabetes. Chickweed leaf extract demonstrated antidiabetic effects, such as lowering blood sugar and hemoglobin A1c in mouse models.
Heart problems in people with diabetes. Chickweed tea given to diabetic rats did not improve their blood sugar levels but did seem to protect against cardiomyopathy.
Anxiety. Chickweed given to mice showed similar activity as diazepam, a classic anxiety medication in the benzodiazepine family.
Here I’ll outline a model of the optimal protein consumption bundle. What does this mean? This means consuming the quantities of protein sources that satisfy the recommended daily intake (RDI) of the essential amino acids and doing so at the lowest possible expenditure. Clearly, this post includes a mix of both nutrition and economics. Since a comprehensive evaluation that includes all possible foods would be a heavy lift, here I’ll just outline the method with a small application.
Consider a list of prices for 100 grams of Beef, Eggs, and Pork.* We can also consider a list that identifies the quantity that we purchase in terms of hundreds of grams. Therefore, the product of the two yields the total that we spend on our proteins.
Of course, not all proteins are identical. We need some characteristics by which to compare beef, eggs, and pork. Here, I’ll use the grams of essential amino acids in 100 grams of each protein source. Because there are different RDIs for each amino acid, I express each amino acid content as a proportion of the RDI (represented by the standard molecular letter).
Then, we can describe how much of the RDI of each amino acid that a person consumes by multiplying the amino acid contents by the quantities of proteins consumed.
Our goal is to find the minimum expenditure, B, by varying the quantities consumed, Q, such that the minimum of C is equal to one. If the minimum element of C is greater than one, then a person could consume less and spend less while still satisfying their essential amino acid RDI. If the minimum element is less than one, then they aren’t getting the minimum RDI.
How do we find such a thing? Well, not algebraically, that’s for sure. I’ll use some linear programming (which is kind of like magic, there’s no process to show here).
The solution results in consuming only 116.28 grams of Pork and spending $1.093 per day. The optimal amino acid consumption is also below. Clearly, prices change. So, if eggs or beef became cheaper relative to pork, then we’d get different answers.
In fact, we have the price of these protein sources going back almost every month to 1998. While pork is exceptionally nutritious, it hasn’t always been most cost effective. Below are the prices for 1998-2025. See how the optimal consumption bundle has changed over time – after the jump.
Since I have posted on the recreational drugs/painkillers kava and kratom for the past two weeks (here and here), I figured I would round it out with a look at the various active compounds that can be derived from the cannabis plant. I knew of THC (the main psychoactive ingredient in weed) and CBD (very tame), but there are many others. When I visited that head shop/kava bar in Florida last month, I noted that they sold a lot of products containing THC-A, THC-P, and HHC, since THC sale is illegal there:
“Super Looper” Vapes, Containing Cannabinoids
The stork clerk showed me the following road-map (with its color-coded “Measure Your Mellow” legend) of various cannabinoids, taking you from innocuous CBD (“Non-psychoactive, soothes anxiety, anti-inflammatory; calming, relaxing”) to THC-P (“Very psychoactive, best entourage effect; energizing, euphoric, total head and body high”) and HHC-P (“Strongest and longest-lasting psychoactive effect; energizing, sativa-like effect”):
Road-Map of Cannabinoids, with putative effects.
On this roadmap, the main “THC” ingredient in weed is shown as Delta-9 or trans-delta-9-Tetrahydrocannabinol (rated as “Very Psychoactive”).
I don’t want to go too far down this rabbit-hole, but out of curiosity I looked up a few articles to try to understand this zoo of mind-altering compounds. Out of sheer laziness, I’ll start with Wikipedia’s take on the pharmacology, focusing on THC itself:
When THC enters the blood stream and reaches the brain, it binds to cannabinoid receptors. The endogenous ligand of these receptors is anandamide, the effects of which THC emulates. This agonism of the cannabinoid receptors results in changes in the levels of various neurotransmitters, especially dopamine and norepinephrine, which are closely associated with the acute effects of cannabis ingestion, such as euphoria and anxiety. Some effects may include a general altered state of consciousness, euphoria, relaxation or stress reduction, increased appreciation of the arts, including humor and music, joviality, metacognition and introspection, enhanced recollection (episodic memory), and increased sensuality, sensory awareness, libido, and creativity. Abstract or philosophical thinking, disruption of linear memory and paranoia or anxiety are also typical. Anxiety is cannabis’s most commonly reported adverse side effect. Up to 30 percent of recreational users experience intense anxiety and/or panic attacks after smoking cannabis….Cannabidiol (CBD), another cannabinoid found in cannabis, has been shown to mitigate THC’s adverse effects, including anxiety.
Cannabis produces many other subjective effects, including increased enjoyment of food taste and aroma, and marked distortions in the perception of time. At higher doses, effects can include altered body image, auditory or visual illusions, pseudohallucinations, and ataxia from selective impairment of polysynaptic reflexes. In some cases, cannabis can lead to acute psychosis and dissociative states such as depersonalization and derealization.
Regarding some other cannabinoids:
There are similar compounds in cannabis that do not exhibit psychoactive response but are obligatory for functionality: cannabidiol (CBD), an isomer of THC; cannabivarin (CBV), an analog of cannabinol (CBN) with a different side chain, cannabidivarin (CBDV), an analog of CBD with a different side chain, and cannabinolic acid. CBD is believed to regulate the metabolism of THC by inactivating cytochrome P450 enzymes that metabolize drugs; one such mechanism is via generation of carbon monoxide (a pharmacologically active neurotransmitter) by upon metabolism of CBD.[14] THC is converted rapidly to 11-hydroxy-THC, which is also pharmacologically active, so the euphoria outlasts measurable THC levels in blood.
Almost none of these psychoactive compounds are present in the raw cannabis plant. The raw plant contains THC-A, which is then converted to THC and CBD, etc., by heating (e.g. by the heat of burning the dried leaves in a joint, or by baking in brownies). THC-A itself seems to have some attractive anti-inflammatory properties. This NIH article has a listing of the major classes of cannabinoids along with a description of their chemistries. Various synthetic cannabinoids have also been created, with some them now included in pharmaceutical preparations. I have not dug into all the research, but it seems likely to me that some combination of these other cannabinoids might have more favorable effects than plain old THC.
Although CBD is not itself psychoactive, it appears to helpfully modulate the effects of THC, and to have its own useful properties. It is used to treat seizures, and possibly anxiety and chronic pain. It can be eaten (think: gummy bears) or applied in skin patches (for longest-lasting, controlled exposure) or oils or lotions. Some varieties (e.g. “Full-Spectrum”) of CBD contain traces of THC, and so act more strongly.
Taking cannabinoids via a tincture under the tongue (where it can cross a mucous membrane, into the bloodstream) takes longer than smoking to show effects, but they last longer. It also gives a more precise dosage, and avoids smoke inhalation, so this seems like a preferable route if it is available. I recall reading some months back that a mixture of THC and CBD taken sublingually was effective in controlling pain. Eating cannabis, as in “Colorado” brownies, can be problematic: it often takes several hours to take effect (via liver metabolism), so users get impatient and start eating more brownies, and then end up way higher than intended.
Long-term adverse effects of cannabis are controversial. Some researchers claim there are none, but:
There is evidence that long-term use of cannabis increases the risk of psychosis, regardless of confounding factors, and particularly for people who have genetic risk factors. A 2019 meta-analysis found that 34% of people with cannabis-induced psychosis transitioned to schizophrenia. This was found to be comparatively higher than hallucinogens (26%) and amphetamines (22%).
Long-term cannabis users are at risk for developing cannabinoid hyperemesis syndrome (CHS), characterized by recurrent bouts of intense vomiting and abdominal cramping during or within 48 hours of heavy cannabis use.
Also, a very recent large study found that 63% of long-term heavy cannabis users had significantly reduced brain function for working memory tasks. (I’ll add that I know someone whose trajectory very strongly suggests that exposure to weed in early teens put a permanent crimp in her mental and emotional functioning).
It seems that habitual use of cannabis can result in general “chill” lassitude, which lowers productivity. As one counselor told a friend of mine, “It is true that with weed ‘nothing happens.’ That is just the problem.”
Weed has long been touted as an alternative pain-killer. I know of people who claim benefits here. Most states allow “medical marijuana” for conditions such as chronic pain or nausea. However, its use is still unlawful at the federal level, so weed must be grown in-state and not transported across state lines.
This NIH site summarizes many studies on cannabis for pain. The evidence is very mixed. Often a significant fraction of subjects report improvements, but so do those on placebos.
My totally amateur takeaway from this flyover: THC and related cannabinoids have a variety of effects on the mind, mostly pleasant but sometimes bad or very bad. There seems little evidence for adverse effects of weed on the body (outside of the brain), but real dangers of messing up your brain with heavy or extended use. As usual with these recreational drugs, harmful interactions are very likely if other substances are used at the same time.
As for pain treatment, it’s effectiveness seems to vary a lot among individuals. Weed may be worth a try as an alternative to opioids, but it still carries significant dangers
If I had to pick a poison for myself as alternative painkiller, at this point it would be a tie between weed (which messes with your brain, not so much your body), and kava (whose side effects mainly show in body parts like the liver and the skin, plus brief nausea). I would experiment to see what worked for me. But first I would make every effort to treat pain through some other means. There are many possible treatments for pain which may be safer than cannabis, and new treatments keep coming. For instance, a friend with neuropathy told me that he experienced relief with a new medicine called Neuropaway.
Huge Disclaimer: I have no expert knowledge here. Don’t act on anything here. All I have done is summarize a few articles. Consult your doctor before doing anything.
P.S.
I could not resist taking a look at the side-effects of drinking alcohol. After all, we all do it, and we have all seen headlines claiming health benefits of drinking a glass of red wine a day. Well, the medical community is pretty down on drinking, saying the proven harms far outweigh the few, slight proven benefits. Even “moderate” consumption can overtax the liver, which really damages it, per this.

















{kind=link}