I knew getting involved in politics was a great way to make enemies, but it never occurred to me until I saw it in action that it can also be a way to make friends.
I’m still not very involved, even as academics go. I think many of us are a bit too eager to talk about political issues in general, but too slow to engage with the policy process in areas directly tied to our research. It’s hard to keep track of every relevant bill and proposed regulation, but I think we bring the most value when we’re the 3rd person to weigh in to share what the research says on an obscure topic, rather than the 3000th person to weigh in on a hot-button issue with a take that sounds just like everyone else on the same side.
My biggest surprise when testifying in state legislatures or public hearings has been that friends follow through while opponents don’t. People who disagree with me will say so at the time, then leave it at that. But people who agree with me will follow up afterwards with messages like “thanks for saying that” or “let’s get coffee”, or let me know when related issues come up.
Perhaps this is unusual, just some good luck in a small sample size, or a reflection of the fact that I only weigh in on relatively obscure issues far from the culture war. But again, I never even thought of this as a possibility. I still wouldn’t run for office any time soon. But if this wasn’t already obvious to everyone else, I encourage you to add this as one term in your own equation as you weigh the pros and cons of political engagement: “nudge the policy process in directions you like” + “engagement takes time and energy and makes enemies” + “maybe friends too”.
Iowa recently joined the growing list of states where midwives or obstetricians can open a freestanding birth center without needing to convince a state board that it is economically necessary. The Des Moines Register provides an excellent summary:
A Des Moines midwife who sued the state for permission to open a new birthing center may have lost a battle in court, but ultimately, she has won the war.
Caitlin Hainley of the Des Moines Midwife Collective sought to open a standalone birthing center in Des Moines, essentially a single-family home repurposed with birthing tubs and other equipment needed to give birth in a comfortable, home-like environment.
To do so, the collective alleged in its 2023 lawsuit, would have required going through a lengthy, expensive regulatory process that would give already established maternity facilities, such as local hospitals, the chance to argue against granting what is known as a certificate of need for the new facility, essentially vetoing competition.
A federal district judge ruled in November that Iowa’s certificate-of-need law is constitutional, finding that legislators had a rational interest in protecting existing hospitals and health care providers.
But while losing the first round in court, the collective’s cause was winning support in a more important venue: the Iowa Capitol. Iowa legislators in their 2025 session passed a bill, which Gov. Kim Reynolds signed on May 1, removing birth centers from the definition of health facilities covered by the certificate-of-need law. The law will formally take effect July 1.
I’m honored to have played a small part in this as the expert witness in the lawsuit.
If you’d like to get involved in making sure birth options are available your state, a great place to start would be to attend the Zoom seminar Roadmap For Reform: Advancing Birth Freedom on July 23rd. It is hosted by the Pacific Legal Foundation, which represented the midwives pro-bono in the Iowa case.
There is strong momentum here with Connecticut, Kentucky, Michigan, Vermont, and West Virginia also recently repealing Certificate of Need requirements for birth centers, but a variety of other barriers remain. States often require freestanding birth centers to obtain a transfer agreement with a nearby hospital before opening to ensure that the hospital will take their emergency cases, even though hospitals are legally required to take all emergency cases. The problem is that hospitals provide both complementary services (emergency care) and substitute services (labor and delivery), and they often choose not to sign transfer agreements in order to prevent competition from a partial substitute. This whole area would benefit both from more academic study, as well as more investigation from antitrust enforcement.
But for today, congratulations to Caitlin Hainley and to Iowa on their victory.
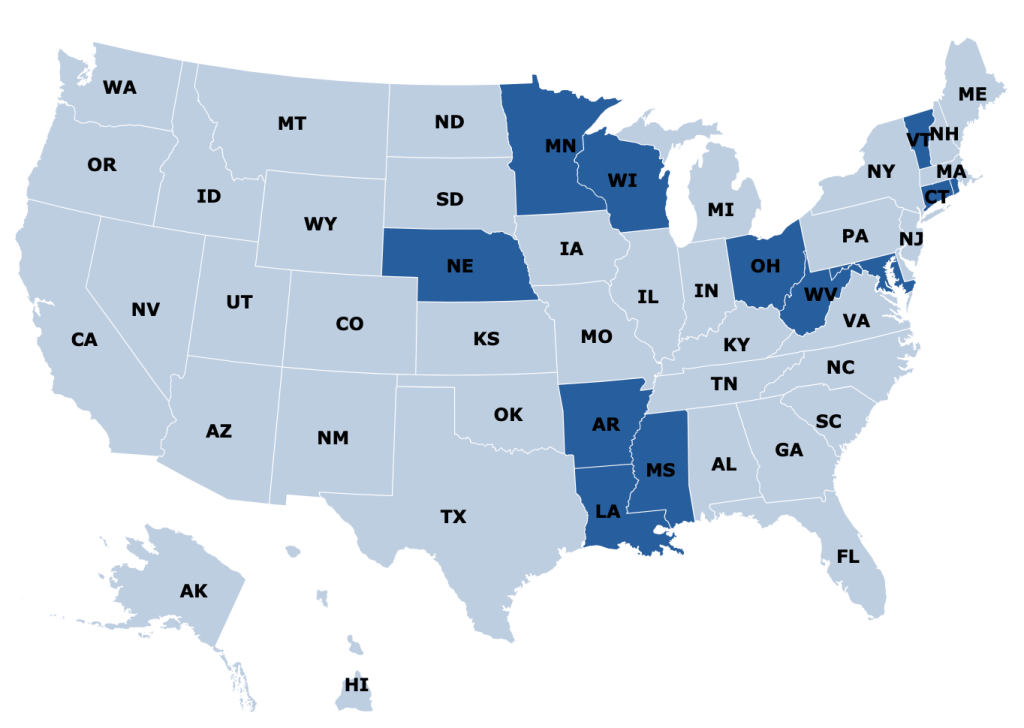
Certificate of Need laws require many types of health care providers to obtain the permission of a state board before they are allowed to open or expand in many US states. But there is a lot of variation from state to state in which types of providers are covered by these laws. I put together this map to show the 15 states that require new home health care agencies to obtain a Certificate of Need:
CON states see reduced competition, which tends to be bad news for patients and new entrants, but good for existing providers and the private equity firms consideringbuying them.
But some CON states like Rhode Island have proposed reforms that would exempt home health agencies from the CON process, putting them in line with the majority of states that put new entrants on an even footing with incumbent providers.
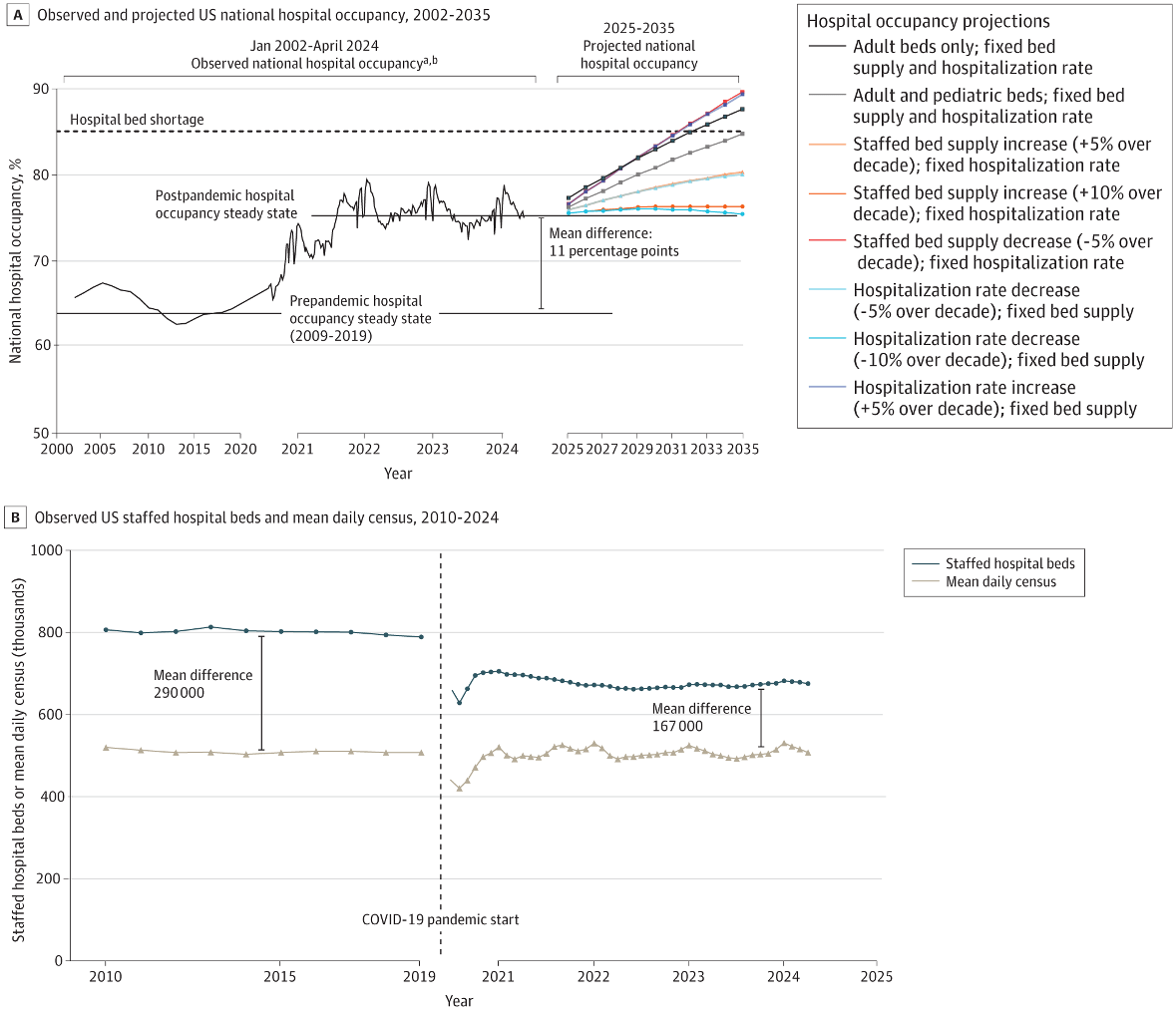
The average hospital is now 3/4 full- more full than during much of the worst of the Covid pandemic, and well above the 2/3 occupancy rate that prevailed during the 2010s. This is according to a study out yesterday in JAMA Open:
This seems to be due to a reduction in bed supply, rather than an increase in demand:
The number of staffed hospital beds declined from a prepandemic steady state of 802 000 (2009-2019 mean) to a post-PHE steady state of 674 000, whereas the mean daily census steady state remained at approximately 510 000
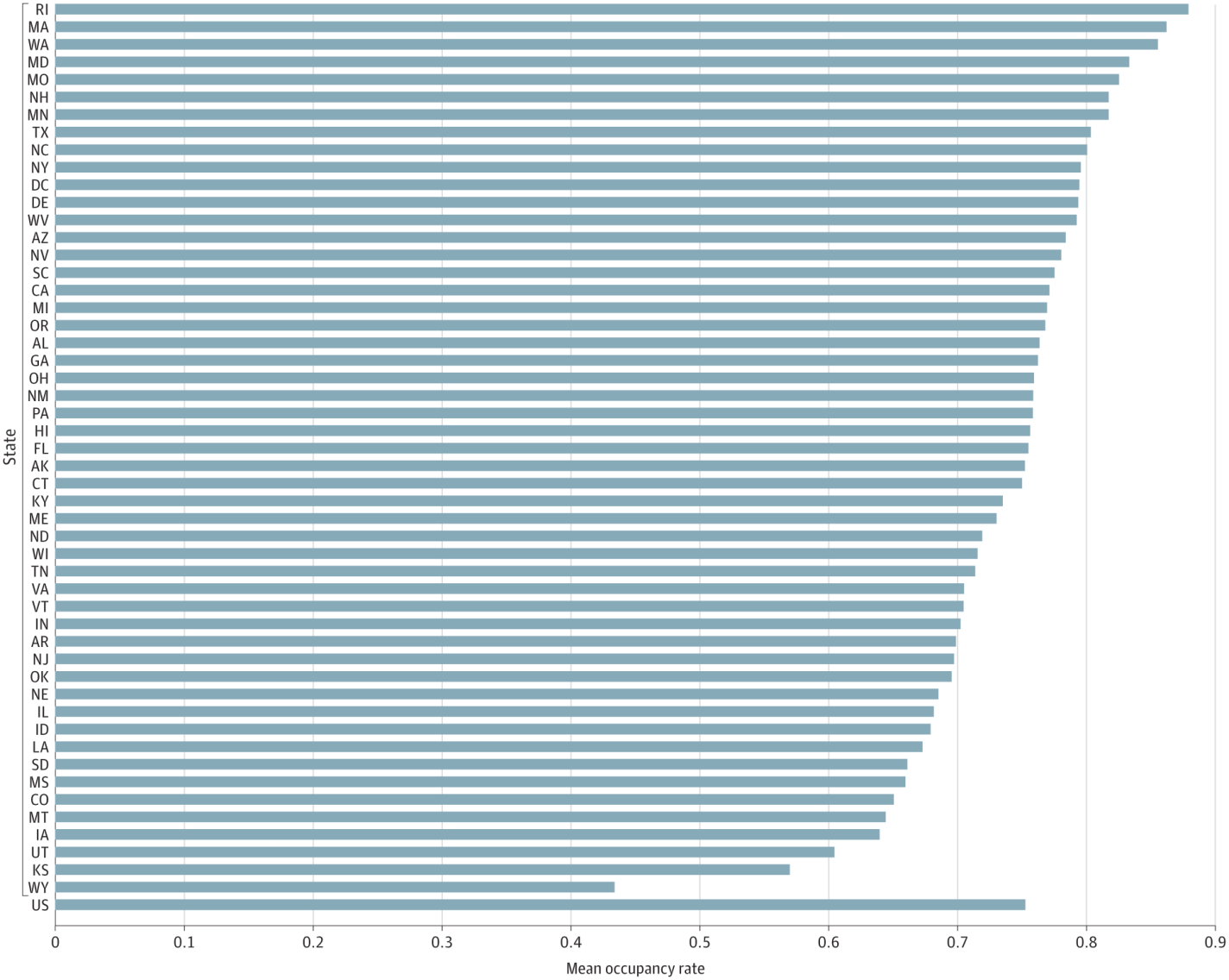
To me this is one more reason to reform Certificate of Need laws that put barriers in the way of hospitals opening or adding beds. Luckily I see a lot of momentum for CON reform this legislative season, including the highest-occupancy state, Rhode Island:
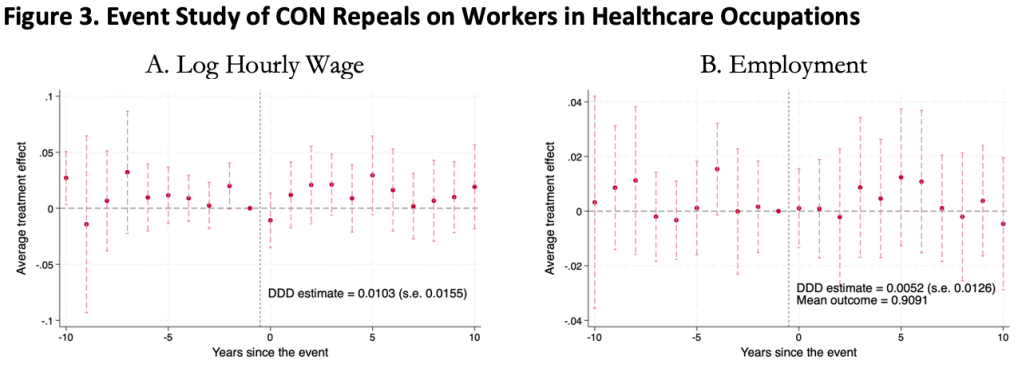
This was surprising to me, as I kind of expected CON laws to harm workers. Certificate of Need laws require many types of health care providers to obtain the permission of a state board before they are allowed to open or expand. This could lead to fewer health care facilities, and so less demand for health care workers, lowering wages and employment. It could also lead to less competition among health care employers, to similar effect.
On the other hand, less competition in the market for health services could raise profits, with room to share them in the form of higher wages. Or, CON being primarily targeted at capital expenditures like facilities and equipment could increase the demand for labor (to the extent that labor and capital are substitutes in health care). All these competing theories seem to cancel out to one big null when we look at the data.
We use 1979-2019 data from the Current Population Survey and a generalized triple-difference approach comparing CON-repealing to CON-maintaining states, and find a bunch of fairly precise zeroes. This holds for many different definitions of “health care worker”: those who work in the health industry, in health occupations, in hospitals, in health care outside hospitals, nurses, physicians, and more.
This is the first word on the topic, not the last; I wouldn’t be too surprised if someone down the road finds that CON does significantly affect health care workers. In this paper we pushed hard on the definition of “health care workers”, but not on “Certificate of Need” or “wages”. We simply classify states as “CON” or “non-CON” because that is what we have data for, but some states have much stricter programs than others, and some day someone will compile the data on this back to the 1970’s. The easier thread to pull on is “wages”. We use one good measure (the natural log of inflation-adjusted hourly real wages), but don’t do any robustness checks around it; considering “business income” could be especially important here. It is also possible that CON affects workers in other ways; we only checked wages and employment.
The full paper is here (ungated here) if you want to read more.
I just found out I’ll be receiving a Course Buyout Grant from the Institute for Humane Studies. It will allow me to teach less next year in order to focus on my research on how Certificate of Need laws affect health care workers.
I’m happy about this because I think this research is valuable and time is my main constraint on doing it (especially doing it quickly enough to inform ongoing policy debates in several states). But I’m also happy because I finally got what I consider to be a “true” grant after many rejections.
I’ve received research funding many times before (e.g. Center for Open Science funding for replications), but it was always relatively small amounts that went directly to me. True grants tend to be larger and to be paid directly to the university. That’s the case with the course buyout grant, which essentially pays the university enough that they can hire someone else to teach my class.
I may have lost count but I’m pretty sure this was the 13th “true grant” I have applied for, and the 1st I will actually receive. Academics have to get used to rejection, since we need to publish and decent journals tend to reject 80%+ of the articles they receive. But for some reason I’ve found grants much harder even than that. From some combination of skill, luck, and targeting lower-tier journals than perhaps I could/should, my acceptance rate for journal articles is probably nearing 50%. I expected this to translate over to grants but it absolutely did not, they seem to be a much different ballgame, one I’m still figuring out.
I’d like to share some of those past misses, both to let junior people see the bumpy road behind success (like a CV of failures), and to try to extract lessons from an admittedly small sample. These proposals were not funded, and probably weren’t even close:
Peterson Foundation US 2050
MacArthur Foundation 100 & Change
RI INBRE (2x)
National Institute for Health Care Management (1x, waiting to hear but probably about to be 2x)
What did these failures of mine all have in common? Me, of course. This is not just a truism; in most of these cases I was applying for major grants solo as an assistant professor without previous funding. The usual advice is to work your way up with smaller grants or, preferably, as the collaborator of a senior professor with lots of previous funding who knows how things work. I knew that would be smart but I’ve tended to be at institutions without senior people in similar fields; almost all my research has either been solo or coauthored with students or assistant professors. Even my PhD advisor was a brand-new assistant professor when we started working together. I had good reasons for ignoring the usual advice to work with well-known seniors, and it has mostly served me well, but grants seem to be the exception.
Twice, I think I did come close on grant proposals, and both times it involved help from seniors at other institutions who had lots of previous funding. At one foundation that funds a lot of social science, my senior coauthor and I got glowing external reviews, but the internal committee rejected us on the grounds that we could do the project without their funding. They were right in the sense that we did do project anyway with no funding; it got published and even won a best paper award. But with their funding we would have done it faster and better and they would have gotten credit for it.
I do think it is smart for funders to consider whether the research would happen anyway without them, or whether their funding really improves things. But I think it is rare for funders to actually do this, and taking this rejection as advice probably led me to more rejections. I tried to propose bigger, more ambitious projects that needed expensive data so it was clear that I really needed the funding; but for most funders this probably made things worse. I have since heard several times that people who get lots of funding from major funders like NIH tend to submit proposals for research they have essentially already finished; that is why their proposals can look so thorough, credible, and polished. They then use the funding to work on their next project (and next proposal) instead of what they said it was for. That seems sketchy to me, but it’s certainly ethical to turn the proposal dial back somewhat toward “obviously achievable for me” from “ambitious and expensive”, and that’s what I’ve done more recently.
The other time I came close was with an R03 proposal to the Agency for Healthcare Research and Quality. First I got a not-close rejection, as I mentioned in the big list, where my proposal was “not discussed”. But AHRQ allows resubmission. At the prompting of my (excellent) grants office, I got feedback on the proposal from two kind seniors at other schools who get lots of funding. I rewrote the proposal based on their comments plus the rejection comments (which were actually quite detailed despite it being “not discussed”) and resubmitted it. This went way better- the resubmission got discussed with an impact score of 30 and a percentile of 17. Lower scores are better for AHRQ/NIH so this was pretty good, good enough that it might have been funded in a normal year, but 2019 was a bad year for government funding (though through some weird quirk I never actually got rejected; 4 years later their system still says “pending council review”). Again, the key to getting close was getting detailed feedback from people who know what they are talking about.
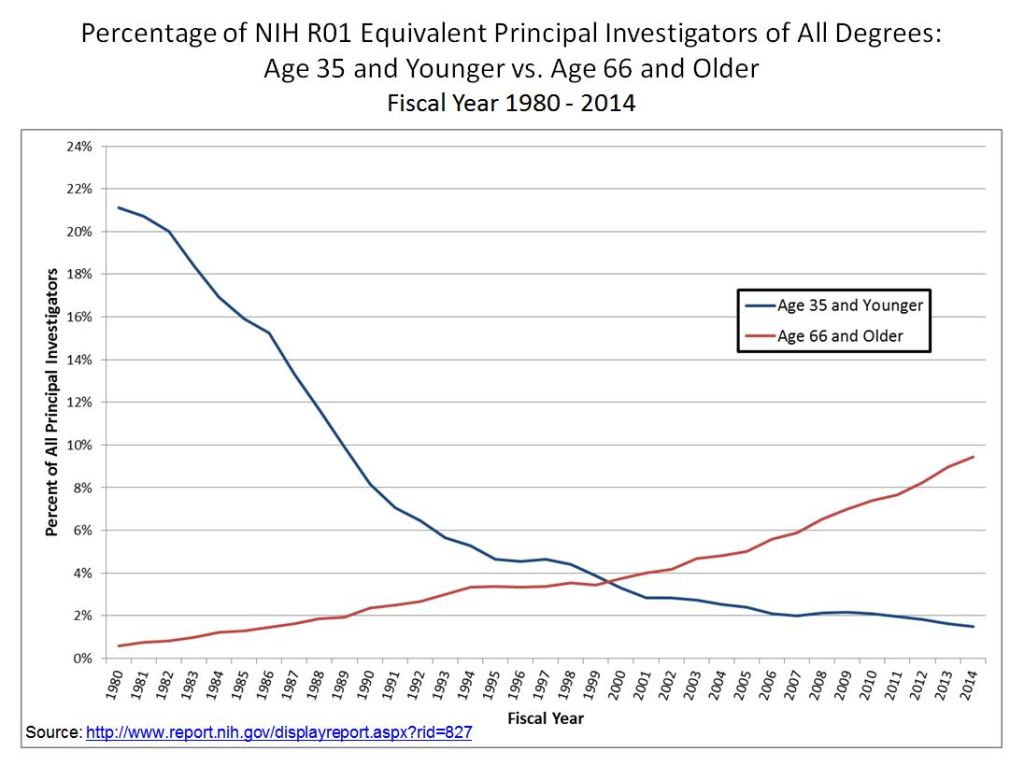
Of course, it also helps to get to know people at the funders and to become more senior yourself. It’s not surprising that my first major grant is coming from IHS given that I’ve been involved with them in all sorts of ways since going to a Liberty & Society seminar way back in 2009. Most funding goes to more senior people who have more connections, knowledge, and proven experience. This is extreme at perhaps the largest funder of research, the National Institutes of Health, where less than 2% of funded principal researchers are under age 36.
This may be the real secret for winning grants- just get older. My 12 rejections all came when I was younger than 36, while my first acceptance came less than a month after my 36th birthday.
In all seriousness, thanks to the Institute for Humane Studies, and I hope that a year from now I’ll be writing here about the great work that came out of this. For everyone with a growing pile of rejections, maybe the 13th time will be the charm for you too.
Last week South Carolina Governor McMaster signed a bill repealing almost all Certificate of Need (CON) laws in the state. If you want to open or expand a health care facility in South Carolina, you can now do so faster, cheaper, and with more certainty.
This is a bigger deal than West Virginia’s reform earlier this year because it applies to almost all types of facilities, and applies to both new facilities and expansions of existing facilities. Only two parts of the CON system remain: a 3-year sunset where hospitals still need special permission to add beds, and a permanent restriction on nursing homes (why? see my recent post on why states hate nursing homes).
As is often the case, this reform took years to enact. I wrote last year about a repeal bill passing the SC Senate; it didn’t make it through the House then, but did this time. As I said then:
This seems like good news; here at EWED we’ve previouslywritten about some of the costs of CON. I’ve written several academic papers measuring the effects of CON, finding for instance that it leads to higher health care spending. I aimed to summarize the academic literature on CON in an accessible way in this article focused on CON in North Carolina.
CON makes for strange bedfellows. Generally the main supporter of CON is the state hospital association, while the laws are opposed by economists, libertarians, Federal antitrust regulators, doctors trying to grow their practices, and most normal people who actually know they exist. CON has persisted in most states because the hospitals are especially powerful in state politics and because CON is a bigger issue for them than for most groups that oppose it. But whenever the issue becomes salient, the widespread desire for change has a real chance to overcome one special interest group fighting for the status quo. Covid may have provided that spark, as people saw full hospitals and wondered why state governments were making it harder to add hospital beds.
Why did reform succeed this time in South Carolina? From where I sit in Rhode Island I can only guess, but here are my guesses. First, the reform side really had their stuff together. See this nice page from SC think tank Palmetto Promise on why to repeal CON, and this paper from Matt Mitchell that does a comprehensive review of the literature on CON and explains what it means for South Carolina. Legislative supporters like Senator Wes Climer just kept pushing.
Second, the biggest opponent of CON reform is usually the state hospital association, but in this case they did not formally oppose repeal. Why not? Here I’m really speculating, but in general it has been faster-growing states that repeal CON. Population growth makes it obvious that new facilities are needed, and it means that existing facilities are thinking about how to grow to take advantage of new opportunities, rather than thinking about lobbying to maintain their share of a static or shrinking pie. You can see some hospital CEOs say they don’t mind repeal in this article (where I’m also quoted). South Carolina has been growing at a decent clip, as is Florida, which also almost-entirely repealed CON in 2019. On this theory, the next big CON reform would happen in a fast-growingCON state like Montana, Delaware, North Carolina, Georgia, or Tennessee. If I had to pick one, I’d say North Carolina.
Update: Apparently Montana already repealed all non-nursing home CON in 2021 and I missed it!
Medicaid is a health insurance program for those with low incomes, funded largely by states. Overall it accounts for less than 20% of US medical spending. But there is one area where it is the dominant payer: nursing homes. Nursing homes are expensive, and Medicare (the typical insurance for those over 65) won’t cover them after the first hundred days, so most nursing home residents end up paying out of pocket until they burn through all their savings and wind up on Medicaid. At which point, Medicaid pays about $100,000 per year to the nursing home for the rest of their life.
States are responsible for up to half of that cost, and so start looking for ways to save money. One idea they have is to make it harder to build nursing homes: if there aren’t beds available, potential nursing home patients will have to stay home instead, where they can’t rack up Medicaid spending the same way. In fact, some states go all the way to a complete moratorium on new nursing homes:
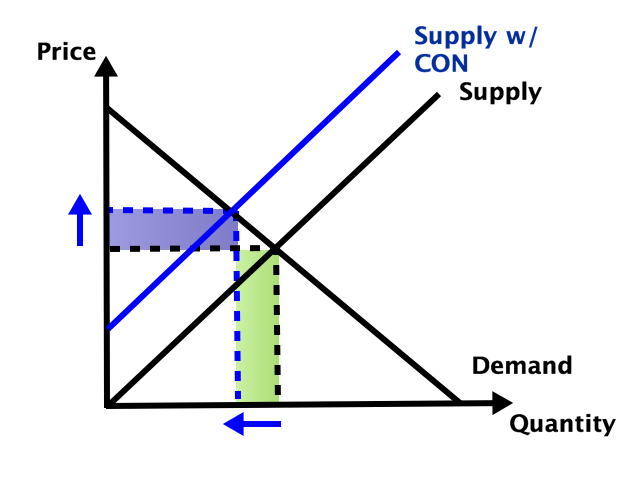
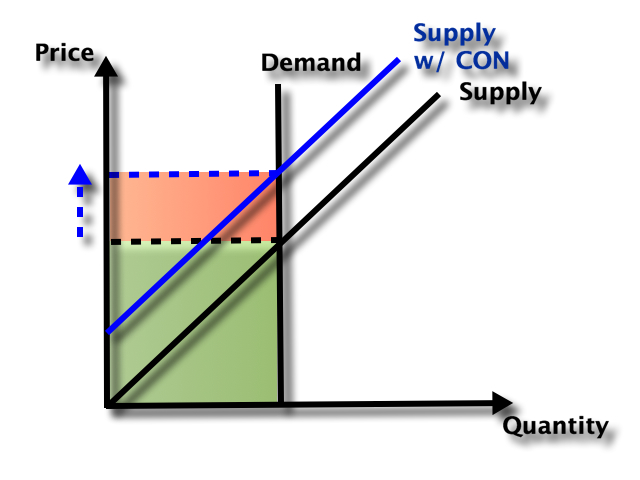
Some other states allow new nursing homes, but only with a special permission slip called a Certificate of Need (CON). CON is often required for other types of health facilities as well, like hospitals or dialysis centers. Research by me and others has generally found that CON doesn’t work as a way to reduce spending, and in fact actually increases it. CON might reduce the number of facilities, but that reduction of supply and competition gives the remaining facilities more power to raise prices.
So which effect dominates- does the smaller number of facilities reduce total spending, or do the higher prices increase it? It depends on the elasticity of demand:
In health care demand is typically quite inelastic, so the price effect dominates, and spending goes up:
But nursing homes could be an exception here. Elasticity of demand could be relatively high because of the number of potential substitutes- home care or assisted living for those with relatively low medical needs, hospitals for those with relatively high medical needs. Plus this is the one type of health care where Medicaid is the dominant payer. They could be especially resistant to price increases here, both due to their market power and their willingness to keep prices so low that facilities won’t take Medicaid patients (another way to save money!).
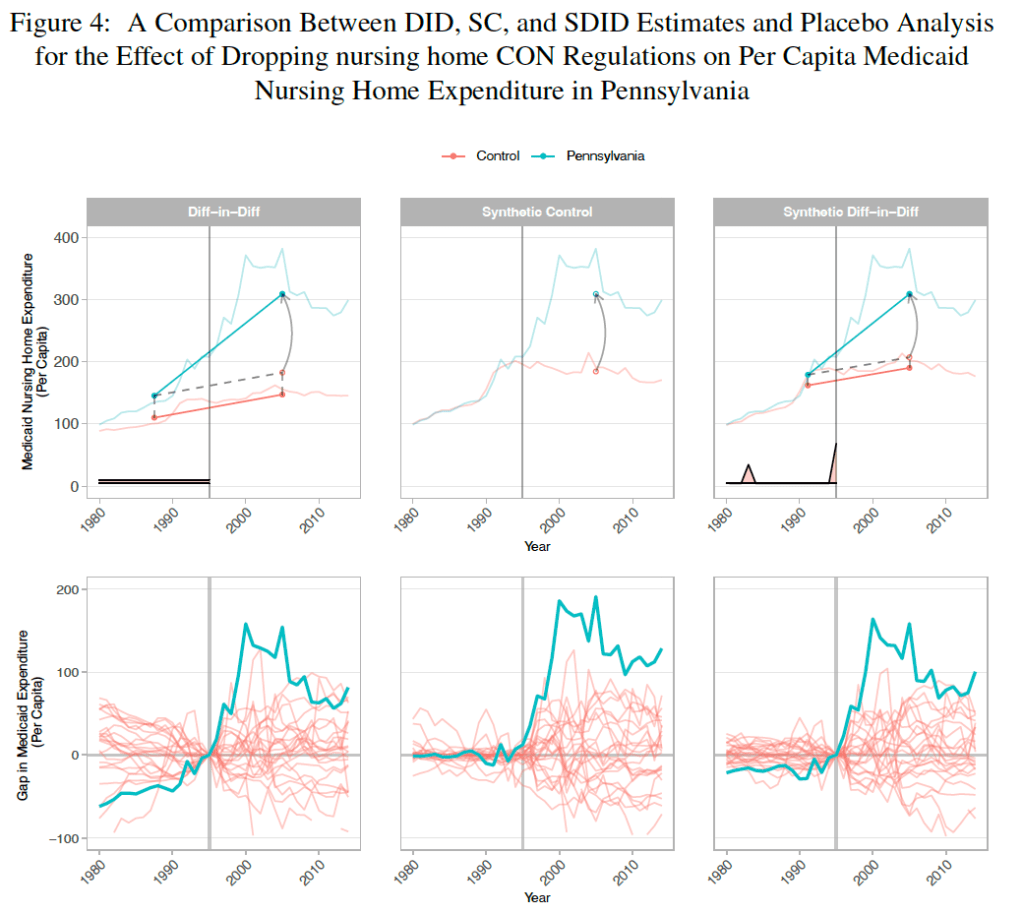
A new paper by Vitor Melo and Elijah Neilson finds that this is indeed the case. Indiana, Pennsylvania, and North Dakota repealed their nursing home CON requirements in the ’90s, and at least for IN and PA their Medicaid spending went way up. The paper uses a new “synthetic difference in difference” technique that seems appropriate, and creates figures that seem confusing at first but get a ton of information across:
They correctly note that they don’t evaluate the welfare effects of the policy; it’s possible that the extra nursing home beds following CON repeal bring huge benefits to seniors that are worth the higher spending. But nursing homes could be the exception to the general rule that CON fails to achieve the goals, like reduced spending, that advocates set for it.
West Virginia just repealed their Certificate of Need requirement for hospitals and birthing centers. Until now anyone wanting to open or expand a hospital needed to apply to a state board for permission. The process took time and money and could result in the board saying “no thanks, we don’t think the state needs another hospital”.
Now anyone wanting to open or expand a hospital and birthing center can skip this step and get to work. This means more facilities and more competition, which in turn leads to lower health care spending relative to trend.
Of course, the rest of West Virginia’s Certificate of Need requirements remain in place; if you want to open many other type of health care facilities, or purchase major equipment like an MRI, you must still get the state board to approve its “necessity”. In some cases, you shouldn’t even bother applying; West Virginia has a Moratorium on opioid treatment programs. Ideally West Virginia would join its neighbor Pennsylvania in a complete repeal of Certificate of Need requirements.
But making it easier to build hospitals and birthing centers is a major step. Hospitals are the largest single component of health spending in the US, and improved facilities might help reduce West Virginia’s infant mortality from its current level as the 4th worst state.
Update 4/7/23: A knowledgable correspondent suggests that the law may only allow existing hospitals to expand without CON (while totally new hospitals would still require one), citing this article. The text of the bill itself seems ambiguous to me. The section “Exemptions from certificate of need” adds “Hospital services performed at a hospital”. For birthing centers by contrast, new construction is clearly now allowed by right: exemptions from CON now include “Constructing, developing, acquiring, or establishing a birthing center”.
I just published a paper on CON laws and spending in Contemporary Economic Policy. As frequent readers of this blog will know, CON laws in 34 states require healthcare providers in 34 US states to get permission from a state board before opening or expanding, and one goal of the laws is to reduce health care spending. The contribution we aim for in this paper is to lay out a theoretical framework for how these laws affect spending.
There have been many empirical papers on this, typically finding that CON laws increase spending, but the only theory explaining why has been simple supply and demand. Health care markets are hard to model for a few reasons, but one big one is that most spending is done through insurers, so the price consumers pay is typically quite a bit lower than the price producers receive. This leads to “moral hazard”- i.e. overuse and overspending by consumers. Normally economists hate monopolies because they lead to underproduction, so in a market with overuse its fair to ask (as Hotelling did about nonrenewable resources)- could two market failures (moral hazard overuse and monopoly underuse) cancel each other out?