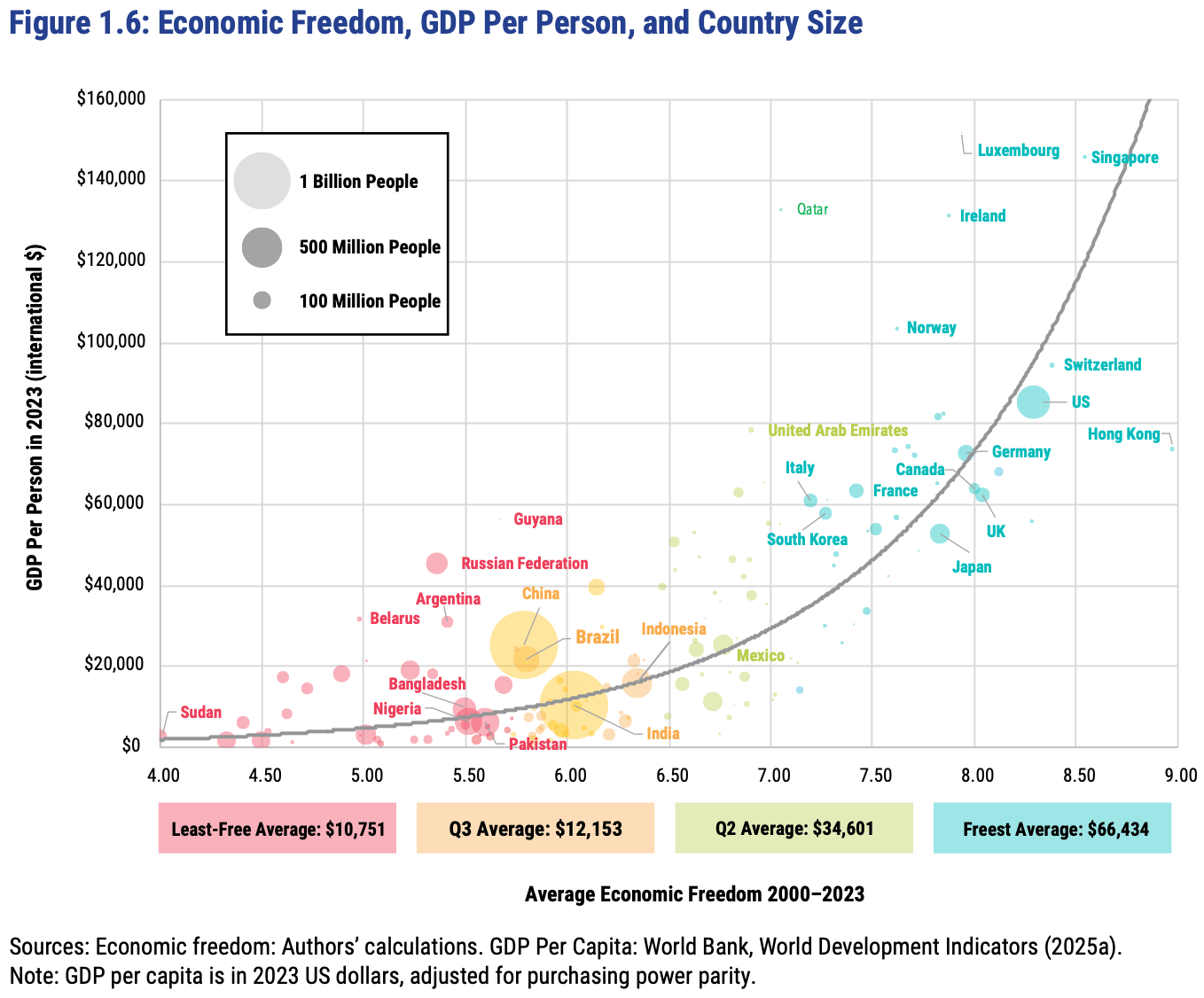
The Fraser Institute released their latest report on the Economic Freedom of the World today, measuring economic policy in all countries as of 2023. They made this excellent Rosling-style graphic that sums up their data along with why it matters:
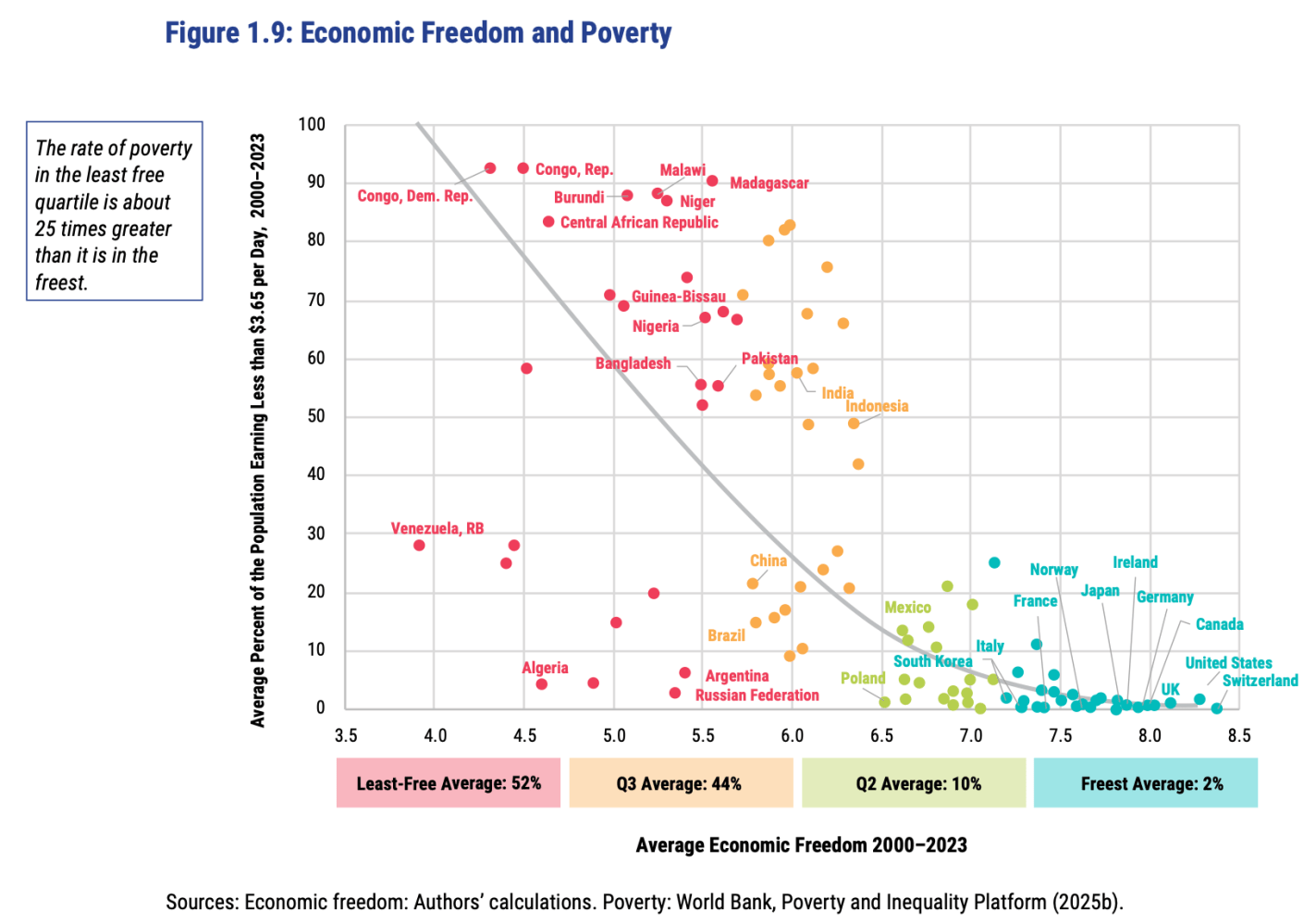
In short: almost every country with high economic freedom gets rich, and every country that gets rich either has high economic freedom or tons of oil. This rising tide of prosperity lifts all boats:
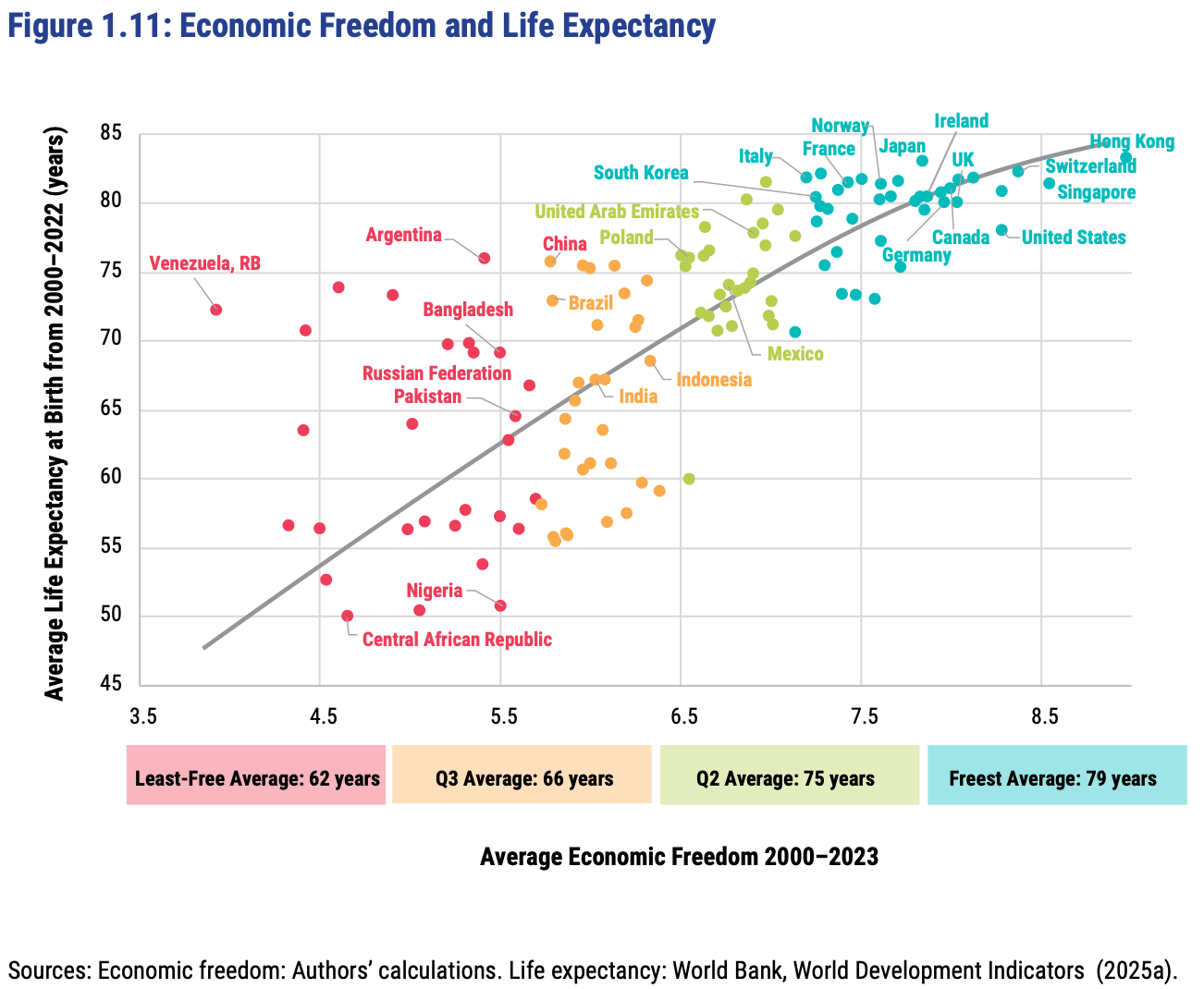
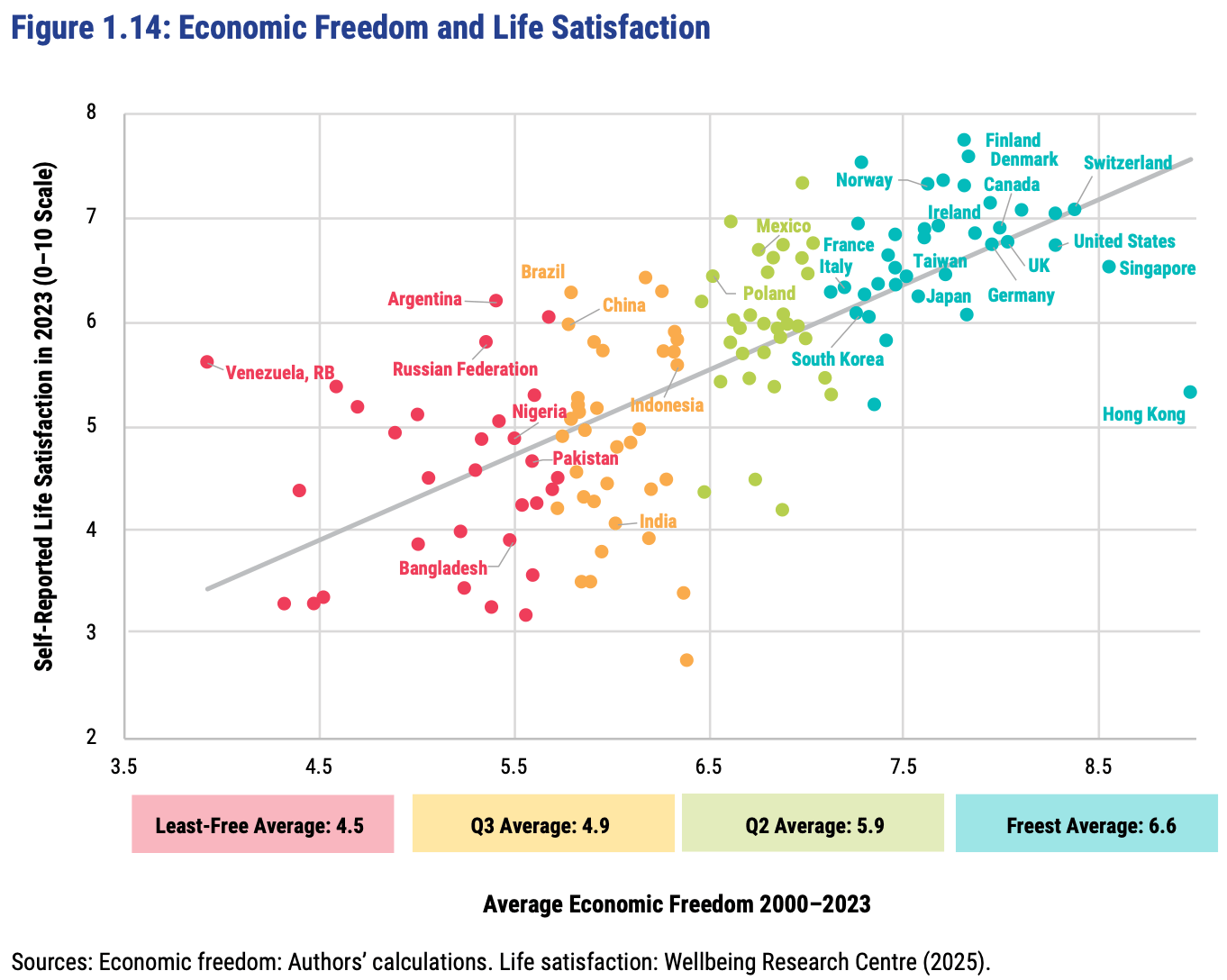
This greater prosperity that comes with economic freedom goes well beyond “just having more stuff”:
The full report, along with the underlying data going back to 1970, is here. The authors are doing great work and releasing it for free, so no complaints, but two additional things I’d like to see from them are a graphic showing which countries had the biggest changes in economic freedom since last year, and links to the underlying program used to create the above graphs so that readers could hover over each dot to identify the country (I suppose an independent blogger could do the first thing as easily as they could…).
FRDM is an ETF that invests in emerging markets with high economic freedom (I hold some), I imagine they will be rebalancing following the new report.
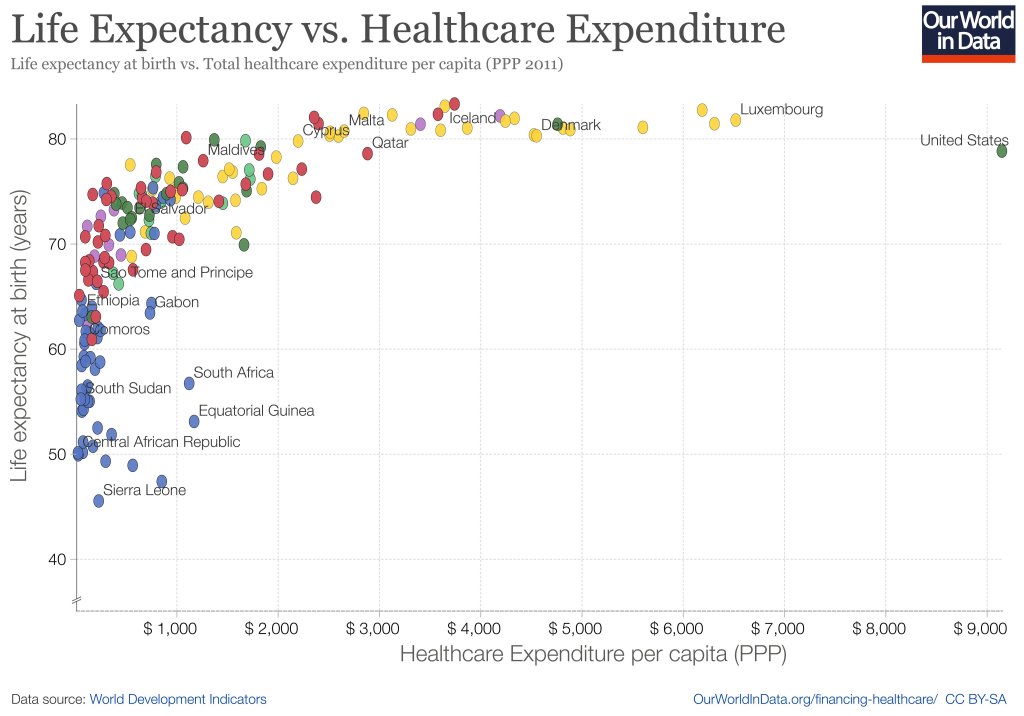
When you look across countries, it appears that the first $1000 per person per year spent on health buys a lot; spending beyond that buys a little, and eventually nothing. The US spends the most in the world on health care, but doesn’t appear to get much for it. A classic story of diminishing returns:
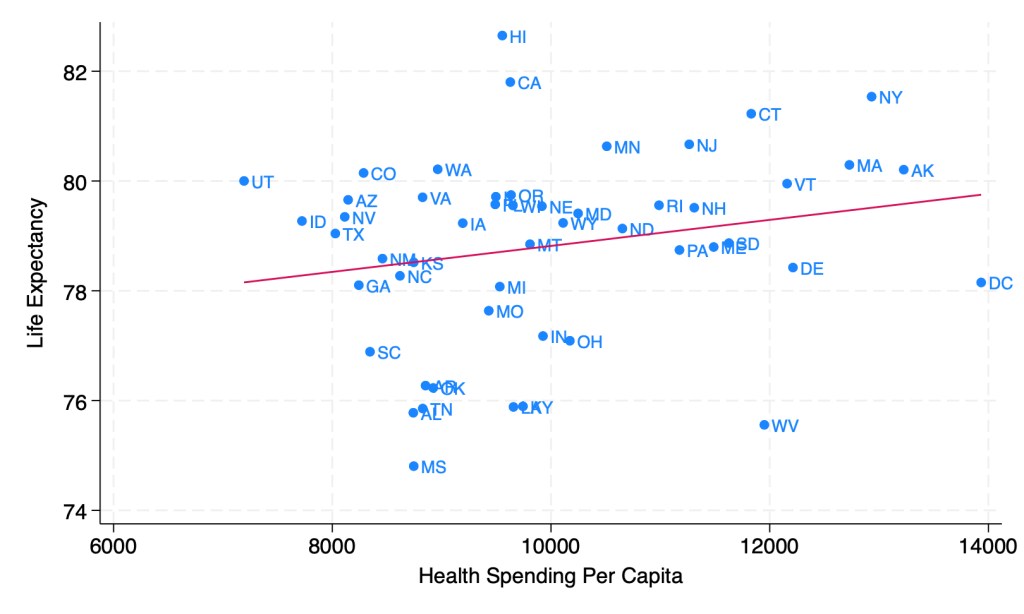
This might tempt you to go full Robin Hanson and say the US should spend dramatically less on health care. But when you look at the same measures across US states, it seems like health care spending helps after all:
Source: My calculations from 2019 IHME Life Expectancy and 2019 KFF Health Spending Per Capita
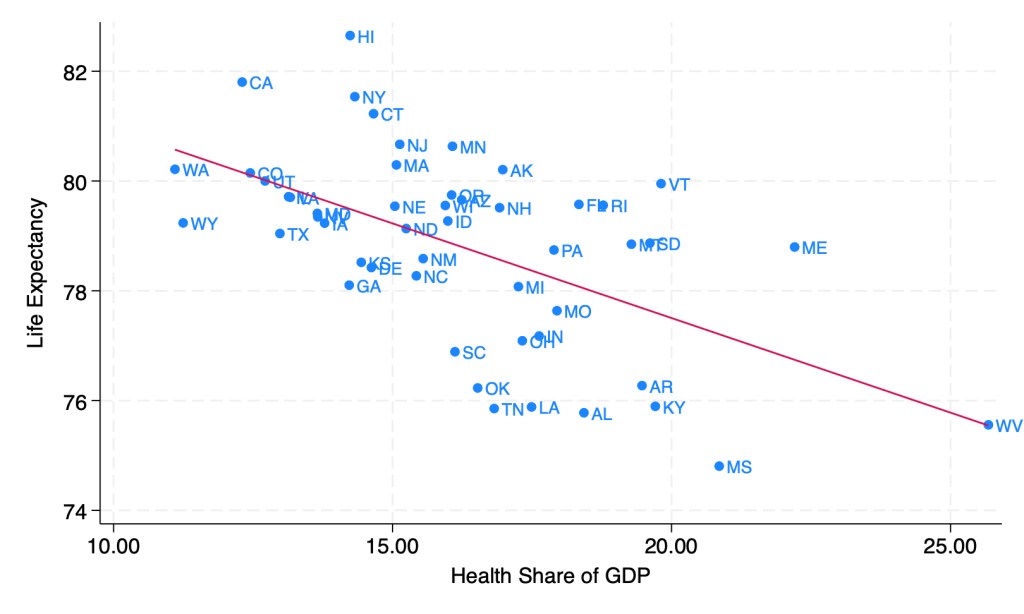
Last week though, I showed how health spending across states looks a lot different if we measure it as a share of GDP instead of in dollars per capita. When measured this way, the correlation of health spending and life expectancy turns sharply negative:
Source: My calculations from 2019 IHME life expectancy, Gross State Product, and NHEA provider spending
Does this mean states should be drastically cutting health care spending? Not necessarily; as we saw before, states spending more dollars per person on health is associated with longer lives. States having a high share of health spending does seem to be bad, but this is more because it means the rest of their economy is too small, rather than health care being too big. Having a larger GDP per capita doesn’t just mean people are materially better off, it also predicts longer life expectancy:
Source: My calculations from 2019 IHME life expectancy and 2019 Gross State Product
As you can see, higher GDP per capita predicts longer lives even more strongly than higher health spending per capita. Here’s what happens when we put them into a horse race in the same regression:
The effect of health spending goes negative and insignificant, while GDP per capita remains positive and strongly significant. The coefficient looks small because it is measured in dollars, but what it means is that a $10,000 increase in GDP per capita in a state is associated with 1.13 years more life expectancy.
My guess is that the correlation of GDP and life expectancy across states is real but mostly not caused by GDP itself; rather, various 3rd factors cause both. I think the lack of effect of health spending across states is real, between diminishing returns to spending and the fact that health is mostly not about health care. Perhaps Robin Hanson is right after all to suggest cutting medicine in half.
Demography is cool generally, but life tables are really cool in their elegance. Don’t know what a life table is? Let me ‘splain.
A life table uses data from private or public death registers, or even genealogical records, to identify a variety of survival and death estimates. Briefly, the tables include for each age:
Probability of death in the next year
Probability of surviving to the age
The life expectancy
There is more in the tables, but these are the big items that people often want to know. All of the various table columns can be calculated from survival rates. The US government and the UN each has created many such tables for a variety of time, locations, and development details. For example, the earliest and most dependable one is from 1901 and includes separate tables by race, sex, migrant status, urbanity, and even for some specific states.
It covers the years 1990 to 2019 for every US state, and has life expectancy at birth, age 25, and age 65. It includes breakdowns by sex and by race and ethnicity, though the race and ethnicity breakdowns aren’t available for every state and year.
This is one of those things that you’d think would be easy to find elsewhere, but isn’t. The CDC’s National Center for Health Statistics publishes state life expectancy data, but only makes it easily available back to 2018. The United States Mortality DataBase has state life expectancy data back to 1959, but makes it quite hard to use: it requires creating an account, uses opaque variable names, and puts the data for each state into a different spreadsheet, requiring users who want a state panel to merge 50 sheets. It also bans re-sharing the data, which is why the dataset I present here is based on IHME’s data instead.
The IHME data is much more user-friendly than the CDC or USMDB, but still has major issues. By including lots of extraneous information and arranging the data in an odd way, it has over 600,000 rows of data; covering 50 states over 30 years should only take about 1,500 rows, which is what I’ve cleaned and rearranged it to. IHME also never actually gives the most basic variable: life expectancy at birth by state. They only ever give separate life expectancies for men and women. I created overall life expectancy by state by averaging life expectancy for men and women. This gives people any easy number to use, but a simple average is not the ideal way to do this, since state populations aren’t exactly 50/50, particularly for 65 year olds. If you’re doing serious work on 65yo life expectancy you probably want to find a better way to do this, or just use the separate male/female variables. You might also consider sticking with the original IHME data (if its important to have population and all cause mortality by age, which I deleted as extraneous) or the United States Mortality DataBase (if you want pre-1990 data).
Overall though, my state life expectancy panel should provide a quick and easy option that works well for most people.
Here’s an example of what can be done with the data:
If states are on the red line, their life expectancy didn’t change from 1990 to 2019. If a state were below the red line, it would mean their life expectancy fell, which done did (some state names spill over the line, but the true data point is at the start of the name). The higher above the line a state is, the more the life expectancy increased from 1990 to 2019. So Oklahoma, Mississippi, West Virginia, Kentucky and North Dakota barely improved, gaining less than 1.5 years. On the other extreme Alaska, California, New York improved by more than 5 years; the biggest improvement was in DC, which gained a whopping 9.1 years of life expectancy over 30 years. My initial thought was that this was mainly driven by the changing racial composition of DC, but in fact it appears that the gains were broad based: black life expectancy rose from 65 to 72, while white life expectancy rose from 77 to 87.
The United States, by far the richest country in the Americas, had a life expectancy of 78.4 years that was falling even before Covid.
How is it that Costa Rica outperforms not only the much richer United States, but also other somewhat richer countries like Panama, Mexico, Argentina, and the Dominican Republic?
Clearly they don’t do it by outspending us- Costa Rica spends the equivalent of $1600 dollars per person per year on health care, compared to nearly $12000 in the US (7.3% of their GDP goes to health care vs 16.8% for the US).
He argues that the key has been Costa Rica’s investment in primary care and public health. The US might may have many more of the world’s best (and most expensive) hospitals, but the easiest and cheapest health benefits come from keeping people out of hospitals in the first place.
the country has made public health—measures to improve the health of the population as a whole—central to the delivery of medical care. Even in countries with robust universal health care, public health is usually an add-on; the vast majority of spending goes to treat the ailments of individuals. In Costa Rica, though, public health has been a priority for decades.
In the nineteen-seventies, Costa Rica identified maternal and child mortality as its biggest source of lost years of life. The public-health units directed pregnant women to prenatal care and delivery in hospitals, where officials made sure that personnel were prepared to prevent and manage the most frequent dangers, such as maternal hemorrhage, newborn respiratory failure, and sepsis. Nutrition programs helped reduce food shortages and underweight births; sanitation and vaccination campaigns reduced infectious diseases, from cholera to diphtheria; and a network of primary-care clinics delivered better treatment for children who did fall sick. Clinics also provided better access to contraception; by 1990, the average family size had dropped to just over three children.
The strategy demonstrated rapid and dramatic results. In 1970, seven per cent of children died before their first birthday. By 1980, only two per cent did. In the course of the decade, maternal deaths fell by eighty per cent. The nation’s over-all life expectancy became the longest in Latin America, and kept growing. By 1985, Costa Rica’s life expectancy matched that of the United States.
Gawande goes on to describe how every Costa Rican gets a home visit from a health care worker at least once per year. This is quite the contrast to the US, where even getting primary care doctors to let you see them in their office can be a fight. I moved to Rhode Island last year and this week finally tried getting a primary care doctor here. I looked through the list of doctors covered by my insurance that my insurer said were accepting new patients and started making calls (by the way, why calls? do any doctors book appointments online?). 2 said that they actually weren’t taking new patients. 9 never answered the phone. The 12th doctor I tried, one farther away and lower-rated than I’d like, finally agreed to see me- in 3 months.
For anyone with less free time, determination, or insurance coverage, it would be natural to just give up after the 5th or the 10th “no”. Clearly many Americans do, leading manageable conditions like diabetes or high blood pressure to turn into acute health crises and expensive hospital visits.
I do think individual doctors could do better here by thinking through their appointment process from the patient’s perspective. But at its core this is simply a numbers issue- we don’t have enough primary care doctors to go around. We actually have fewer doctors per capita than Costa Rica, and relatively high share of specialists means that we have even fewer primary care doctors to go around. More medical school spots, more primary care residency spots, and fewer restrictions on immigrant doctors could go a long way way toward helping to US catch up to…. Costa Rica.
That, or their secret is just the volcanoes. This is surprisingly plausible- the US state with the longest life expectancy is also the one best known for volcanoes, Hawaii.