The flu and covid-19 vaccines don’t work super well. Both vaccines permit infection and transmission at quite high rates. The benefit from these vaccines come largely from reductions in mortality or severe symptoms conditional on infection. The covid-19 vaccine is itself especially risky or ineffective depending on the age and health of the individual. Plenty of people eschew vaccines.
I live in Collier County, Florida where there have been 61 confirmed cases of measles so far this year. I have since learned that Measles is EXTREMELY contagious. It floats around the air and on items and just sort of hangs out and waits for a place to replicate. I’ve also learned that symptoms include a fever, eye irritation, possible brain swelling, severe dehydration, and a characteristic rash. The severe dehydration easily puts people in the hospital, the eye irritation can lead to permanent vision loss, and the brain swelling can be acute, or a symptom delayed by 5-6 years, which can also be fatal. I’ve also learned that having the vaccine, which is usually administered in two doses, provides about 97% immunity. The vaccine works so well, that the department of health recommends no behavioral change among the vaccinated population when there is a measles outbreak. Barring unique circumstances, measles immunity can persist for a lifetime.
Unfortunately, a large segment of the anti-vaccine mood affiliation retains the salience of the covid-19 vaccine characteristics. Other vaccines and diseases in the typical pediatric schedule are not similar. Most of these prevent infection >90% of the time (TDAP is low at 73%), prevent transmission, reduce mortality when there are breakthrough infections, are effective for years or decades, and are extremely safe for all age groups.
The risks of disease versus the corresponding vaccine are orders of magnitude away from each other. The tables below summarize the data (with sources). I did not double check the source on every single figure. If you glance below, then you’ll see why: Even if the numbers are closer by 10 or 100 times, vaccines still look really good.
First, mortality: The data is divided by disease and age group, and provides mortality rates for both the disease and for the vaccine. The numbers are proportions, conditional on infection or vaccination. There are a lot of zeros in the vaccine mortality rates and certainly more than for the diseases. For example, a measles infection is 10,000 more lethal than the MMR vaccine which prevents it. In fact, all of those zeros in the vaccine rates reflect mortality that is so uncommon, that the estimated one out of every 10 million is just rounded up because researchers don’t think that the risk is zero.
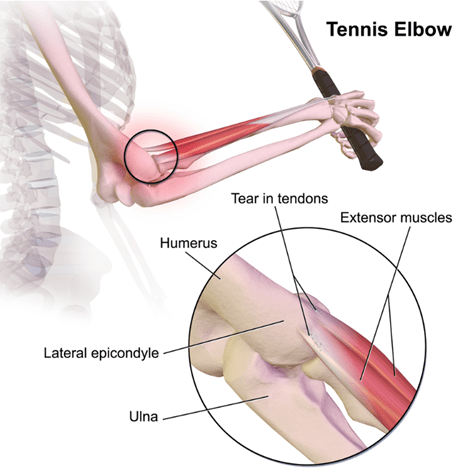
Tennis elbow (or these days, pickleball elbow) is a painful, debilitating condition that affects around 2% of adults at any given time. Active tennis players have about a 50% chance of being stricken at some point. If you give it a chance to heal, it usually goes away within a year, but that is a long time to be in pain or disabled.
The traditional technical name for this condition is “lateral epicondylitis.” That suffix “…itis” implies inflammation, but it is now known that typical inflammation markers are generally absent. So, the new jargon is the deliberately ambiguous “tendinosis” or even “tendinopathy.” It seems to be caused by accumulated damage to the very end of the tendon that anchors the muscles which are attached to the back of your hand. Those muscles that let you tilt your hand up; if you grip something hard and try to hold something steady, those muscles contract in a big way. The micro tears seem to occur right about where that tendon attaches to a little knob of bone at the very outside of your elbow joint:
This condition is somewhat frustrating for doctors and for patients, since there’s not a single clear effective treatment. Although injecting Cortisone type anti-inflammatories gives short-term pain relief, it seems to adversely affect longer term outcomes, so those shots are less common than 20 years ago. Therapists throw all sorts of techniques at it, including NSAIDs, heat, cold, exercises, braces, shock waves, acupuncture, injections of blood extracts, and so on. All these may help, though for every study that shows positive results for a given treatment there seems to be one that doesn’t.
I have a personal interest in this subject, since I have a long-standing for propensity towards tennis elbow. I had to stop playing tennis many years ago because of it. More recently, I spent the day helping on a work project, installing sheet rock to repair flood damage in a someone’s home. After a day gripping a powered drill driver, the old tennis elbow flared up significantly.
In the course of my internet search, I ran across a very promising study that seems to have been largely neglected. It is also a sweet piece of science.
An orthopedist named Jerrold Gorski started reflecting on the common observation that tennis elbow often feels worst upon waking up in the morning. That made him wonder whether something was going on in the night that caused the condition to worsen. Which led him to hypothesize that tennis elbow might be helped by changing a patient’s sleep posture. Prior studies showed that people spend some 55% of the night sleeping with their arm crooked up overhead, something like this:
That position could keep stress on the tendon all night, and inhibit it from healing. Dr. Gorski also noted that in the literature there are other examples of sleep posture or waking postures making a difference in treating various orthopedic conditions.
And so, like a good scientist, he devised an experiment to test his hypothesis. He came up with a very simple technique of using a bathrobe belt, which is soft and wide, to restrain the arm during sleep. You simply tie a large loop at one end that goes around the thigh, and a smaller loop at the other that fits snuggly around the wrist. If all goes well, this rigging well prevent will keep the arm down close to the side all night, so it cannot get crunched under the head:
Dr. Gorski tried tried this out with 39 tennis elbow patients. Six of them apparently could not tolerate being roped for the night, so they were designated as “treatment failures”, or effectively a control group. The other 33 patients stuck with the protocol, although most of them, like the 6 “treatment failures”, complained about interference with going to sleep or staying asleep.
There was a fairly dramatic difference in outcomes. The six treatment failures had ongoing tennis elbow symptoms that persisted unchanged over the initial 3-month study period. Of the thirty-three patients who stuck with the protocol, 66% reported improvement within 1 month, and 100% of them improved within 3 months. Those are really good results.
Obviously, it’s not a perfect study. It only claims to be a prospective study. Nevertheless, the results were so promising, and the treatment was so inexpensive and harmless and noninvasive, I would’ve thought that it would get a lot of attention. But looking in Google Scholar for citations, I only saw seven articles that cited it. Two of those articles were letters to the editor by the author, Dr. Gorksi himself, seemingly trying to draw due attention to his promising study, and one citation was in an article that got retracted. This leaves only 4 independent citations in the medical literature all of which, as best I could tell, were about touting some other treatment, and just nodded in passing to Dr. Gorski’s work. So, essentially crickets. One can only speculate on why the medical profession has not paid more attention to a treatment which requires nothing more than an office visit and demo with a strip of cloth.
I want to give a shout-out to the UK-based “Sports Injury Physio” website, which, in a very helpful and comprehensive article on tennis elbow care, noted:
Sleeping with your elbow straight is usually a gamechanger. There is something about keeping the elbow bent for long periods that irritates tennis elbow and makes the pain worse. It can be a bit challenging to figure out how to keep your elbow straight while tossing and turning in bed, but my patients who manage this report big improvements in their pain.
That endorsement piqued my interest. The Wikipedia article on tennis elbow also mentions this treatment clearly. With my nascent tennis elbow, I decided to try it for myself. Using a bowline knot (which does not slip), I tied a loop at one end of a bathrobe belt just big enough to wriggle my hand through, and a larger loop at the bottom to go around my thigh:
It is somewhat awkward to sleep with this on, but it is entirely bearable if you set your mind to it and plan ahead, e.g., where to position your nighttime tissue box. After only two nights on this protocol, I am now waking up with no pain in my elbow. Thanks, doc.
This will be a longer-than-usual post, since I will try to include all the steps I used to grow salad ingredients in a compact (AeroGarden-type) hydroponics system. I hope this encourages readers to try this for themselves. See my previous post for an introduction to the hardware, including small modifications I made to it. I used a less-expensive ($45), reliable 18-hole MUGFA model here, but all the AeroGardens and its many knockoffs should work similarly. Most plant roots need access to oxygen as well as to water; these hydroponic units allow the upper few inches of the root to sit in a (moist) “grow sponge” up out of the water to help with aerobic metabolism.
Step 1. Unbox the hydroponics unit, set up per instructions near a power outlet. Fill tank close to upper volume marking.
Step 2. Add nutrients to the water in the tank: usually there are two small plastic bottles, one with nutrient mix “A” and the other with nutrient mix “B”, initially as dry granules. Add water to the fill lines of each of these bottles with the granules, shake till dissolved. (You can’t mix the A and B solutions directly together without dilution, because some components would precipitate out as solids. So, you must add first one solution, then the other, to the large amount of water in the tank.)
There is more than one way to do this. I pulled the deck off the tank, used a large measuring cup to get water from my sink into the tank, a little below the full line. For say 5 liters of water, I add about 25 ml of nutrient Solution A, stir well, then add 25 ml of Solution B and stir. You could also keep the deck on, have the circulation pump running, and slowly pour the nutrient solutions in through the fill hole (frontmost center hole in the deck). You don’t have to be precise on amounts.
Step 3. Put the plastic baskets (sponge supports) in their holes in the deck, and put the conical porous planting sponges/plugs in the baskets. Let the sponges soak up water and swell. (This pre-wetting may not be necessary; it just worked for me).
Step 4. Plant the seeds: Each sponge has a narrow hole in its top. You need to get your seed down to the bottom of the hole. I pulled one moist sponge out at a time and propped it upright in a little holder on a table where I could work on it. I used the end of plastic bread tie to pick up seeds from a little plate and poke them down to the bottom of the hole. You have to make a judgment call how many seeds to plant in each hole. Lettuce seeds are large and pretty reliable, so I used two lettuce seeds for each lettuce sponge. Same for arugula (turns out that it was better to NOT pre-soak the arugula seeds, contrary to popular wisdom). If both seeds sprout, it’s OK to have two lettuce plants per hole, though you may not get much more production than from one plant per hole. For parsley*, where I wanted 2-3 plants per hole, I used three seeds each. For the tiny thyme seeds, I used about 5 seeds, figuring I could thin if they all came up. For cilantro, I used two pre-soaked seeds. I really wanted chives, but they are hard to sprout in these hydroponics units. I used five chive seeds each in two holes, but they never really sprouted, so I ended up planting something else in their holes.
I chose all fairly low-growing plants, no basil or tomatoes. Larger plants such as micro-dwarf tomatoes can be grown in these hydroponics units; also basil, though need to aggressively keep cutting it back. It may be best to choose all low or all high plants for a given grow campaign. See this Reddit thread for more discussion of growing things in a MUGFA unit.
Once all the plugs are back in their holders, you stick a light-blocking sticker on top of each basket. Each sticker has a hole in the middle where the plants can grow up through, but they block most of the light from hitting the grow sponge, to prevent algae growth. Then pop a clear plastic seeding cover dome on top of each hole, and you are done. The cover domes keep the seeds extra moist for sprouting; remove the domes after sprouting. Make sure the circulation pump is running and the grow lights are on (typically cycling on 16 hours/off 8 hours). This seems like a lot of work describing it here, but it goes fast once you have the rhythm. Once this setup stage is done, you can just sit back and let everything unfold, no muss, no fuss. Here is the seeded, covered state of affairs:
Picture: Seeds placed in grow sponges on Jan 14. Note green light-blocking stickers, and clear cover domes to keep seeds moist for germination. The overhead sunlamp has a lot of blue and red LEDs (which the plants use for photosynthesis), which gives all these photos a purple cast.
Jan 28 (Two weeks after planting): seedlings. Note some unused holes are covered, to keep light out of the nutrient solution in the tank. The center hole in front is used for refilling the tank.
Feb 6. Showing roots of an arugula plant, 23 days after planting.
Step 5. Maintenance during 2-4 month grow cycle. Monitor water level via viewing port in front. Top up as needed. Add nutrients as you add water (approx. 5 ml of Solution A and 5 ml Solution B, per liter of added water). The water will not go down very fast during the first month, but once plants get established, water will likely be needed every 5-10 days. If you keep trimming outside leaves every several days, you can get away with having densely planted greens, whereas if you only harvest say every two weeks, the plants get so big they would crowd each other if you plant in every hole on the deck.
Optional: Supposedly it helps to keep the acidity (pH) of the nutrient solution in the range of 5.5-6.5. I think most users don’t bother checking this, since the nutrient solutions are buffered to try to keep pH in balance. Being a retired chemical engineer, I got this General Hydroponics kit for measuring and adjusting pH. On several occasions, the pH in the tank was about 6.5. That was probably perfectly fine, but I went ahead and added about 1/8 teaspoon of the pH lowering solution, to bring it down to about 6.0. I also got a meter for measuring Electrical Conductivity/Total Dissolved Solids to monitor that parameter, but it was not necessary.
Feb 16: After a month, some greens are ready to snip the outer leaves. Lettuces (buttercrunch, red oak, romaine) on the right, herbs on the left.
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Feb 17: Harvesting a small salad or sandwich filler every 2-3 days now.
March 6: Full sized, regular small harvests. All the lettuces worked great, buttercrunch is especially soft and sweet. Arugula (from the mustard plant family) gave a spicy edge. Italian parsley and thyme added flavor. The cilantro was slower growing, and only gave a few sprigs total.
Closeup March 16 (three months), just before closing out the grow cycle. Arugula foreground, lettuce top and right, thyme on left, Italian parsley upper left corner.
Step 6. Close out grow cycle. At some point, typically 2-4 months, it is time to bring a grow cycle to a close. I suppose with something like dwarf tomatoes, you could keep going longer, though you might need to pull the deck up and trim the roots periodically. In my case, after three months, the arugula and cilantro were starting to bolt, though the lettuce, thyme, and parsley were still going strong. As of mid-March, my focus turned to outside planting, so I harvested all the remaining crops on the MUGFA, turned off the power, and gently pulled the deck off the tank. The whole space under the deck was a tangled mass of roots. I used kitchen shears to cut roots loose, enough to pull all the grow sponges and baskets out. The sponges got discarded, and the baskets saved for next time. I peeled off and saved the round green light-blocking stickers for re-use. I cleared all the rootlets from the filter sponge on the pump inlet. Then I washed out the tank per instructions. It took maybe 45 minutes for all this clean-out, to leave the unit ready for a next round of growing.
Stay tuned for a future blog post on growing watercress, which went really well this past fall. Looking to the future: In Jan 2026 I plan to do a replant of this 18-hole (blocked down to 14-holes) MUGFA device, sowing less lettuce (since we buy that anyway) but more arugula/Italian parsley/thyme for nutritious flavorings. For replacement nutrients and grow sponges, I got a Haligo hydroponics kit like this (about $12).
Growing these salad/sandwich ingredients in the kitchen under a built-in sunlamp provided good cheer and a bit of healthy food during the dark winter months. The clean hydroponic setup removed concerns about insect pests or under/overwatering. It was a hobby; at this toy scale it did not “save money”, though from these learnings I could probably rig a larger homemade hydroponics setup which might reduce grocery costs. This exercise led to fun conversations with visitors and children, and was a reminder that nearly everything we eat comes from water, nutrients, and light, directly or indirectly.
*Pro tips on germinating parsley seeds – – Parsley seeds have a tough coating, and can take weeks to germinate. Some techniques to speed things up:
( 1 ) Lightly abrade the seeds by gently rubbing between sheets of sandpaper.
( 2 ) Soak in warmish water for 24-48 hours.
( 3 ) For older seeds, cold stratification (1–2 weeks in a damp paper towel in the fridge) may help break dormancy.
By almost any measure, 2025 was a great year for the United States.
Despite inflation remaining elevated and the damage from new tariffs, the economy did well. Inflation-adjusted median earnings are higher than a year ago, though only by about 1.3%. While most prices are still rising, one bright spot for affordability is that home prices are falling in much of the country (according to Zillow estimates).
The unemployment rate did tick up slightly, from 4.2% last November to 4.6% currently. This is definitely an indicator to watch over the next few months, but it is still well below average.
But even outside of the economy, there is plenty of good news in the data. Crime rates are plummeting. The murder rate fell something like 20%, as well as every major category of crime (violent crime overall is down 10%). This are some of the largest one-year drops in crime the US has ever seen.
Homicides aren’t the only category of deaths that are falling in 2025. For most categories of death as tracked by the CDC, there is a long lag (6 months or more) before all of the deaths are categorized. So we can’t look at complete 2025 data yet. For example, drug overdoses have increased massively in recent years, especially during the pandemic. But after plateauing in 2021-23, drug ODs started falling in 2024 and have continued to fall in early 2025. For the 12 months ending in April 2025, drug OD deaths were 26% lower than the prior 12 months. If we look at just the first 5 months of the year, 2024 was 20% lower than 2023, and 2025 was another 20% lower than 2024. For the first five months of 2025, ODs are basically back down to the same level as 2018 and 2019. Motor vehicle deaths also increased during the pandemic, but they are down 8% in the first half of 2025, essentially back down to 2018-19 levels.
Was it all good news? No, you can certainly find some data to be pessimistic about. For example, despite the efforts of DOGE and other attempts to cut federal government spending, over $2 trillion was added to the national debt in 2025, up 6 percent from the end of 2024 and surpassing $38 trillion. And as I mentioned above with the unemployment rate, there is some evidence the labor market may be weakening.
Not all is rosy as we head into 2026, but 2025 was a year filled with many positive trends on the economic front and in society more generally. May your new year be prosperous and healthy!
Merry Christmas! I’m gifting you a couple ideas for money things to do in the remaining six days of 2025.
Ways to Help Yourself
Money in US Flexible Spending Accounts (FSAs) often disappears if not requested by New Year’s Day. Don’t forget to draw these down- especially it is a Dependent Care FSA, which can’t carry any money over to the new year. The money goes back to your employer if you don’t spend it, which means they don’t have an incentive to remind you themselves; so I’ll remind you to save you from having to go Krieger.
The next few days are also your last chance to do most tax-deductible spending in 2025, which could be business expenses, or contributing to tax-deductible accounts that don’t expire like a 401k or HSA (not FSA). See a more detailed list of tax ideas here. Depending on your situation (especially whether you itemize), this might also be a good time to make tax-deductible donations, which would:
Help Others
There are many good causes to donate to, but funding high-value low-cost health interventions in poor countries was probably the cheapest reliable way to save a life even before this year. When one of the largest funders of global health, USAID, was shut down this year, the marginal benefit of donations to global health likely went even higher. Givewell does the cost-effectiveness calculations to identify good options for specific charities in this area, like Helen Keller International. I like that I’ve been donating to these charities for years via Givewell’s donation portal and none of them have ever called me (since they don’t require a phone number) or mailed me anything.
This picture shows all the remains of the website of USAID, an agency that spent $32 billion in FY 2024
Academics generally agree on the changing patterns of mortality over time. Centuries ago, people died of many things. Most of those deaths were among children and they were often related to water-borne illness. A lot of that was resolved with sanitation infrastructure and water treatment. Then, communicable diseases were next. Vaccines, mostly introduced in the first half of the 20th century, prevented a lot of deaths.
Similarly, food borne illness killed a lot of people before refrigeration was popular. The milkman would deliver milk to a hatch on the side of your house and swap out the empty glass bottles with new ones full of milk. For clarity, it was not a refrigerated cavity. It was just a hole in the wall with a door on both the inside and outside of the house. A lot of babies died from drinking spoiled milk.
Now, in higher income countries, we die of things that kill old people. These include cancer, falls that lead to infections, and the various diseases related to obesity. We’re able to die of these things because we won the battles against the big threats to children.
What prompts such a dreary topic?
I was perusing the 1870 Census schedules and I stumbled upon some ‘Schedule 2s’. Most of us are familiar with schedule 1, which asks details about the residents living in a household. But schedule 2 asked about the deaths in the household over the past year. Below is a scan from St. Paul, Minnesota.
Given where we are starting from, the average American would probably be satisfied with a fairly low bar, like “not obese” or “can run a mile without stopping”. But the kind of person who writes about the topic a lot tends to be a fitness nut insisting on crazily high standards. So what makes for a reasonable middle-ground measure?
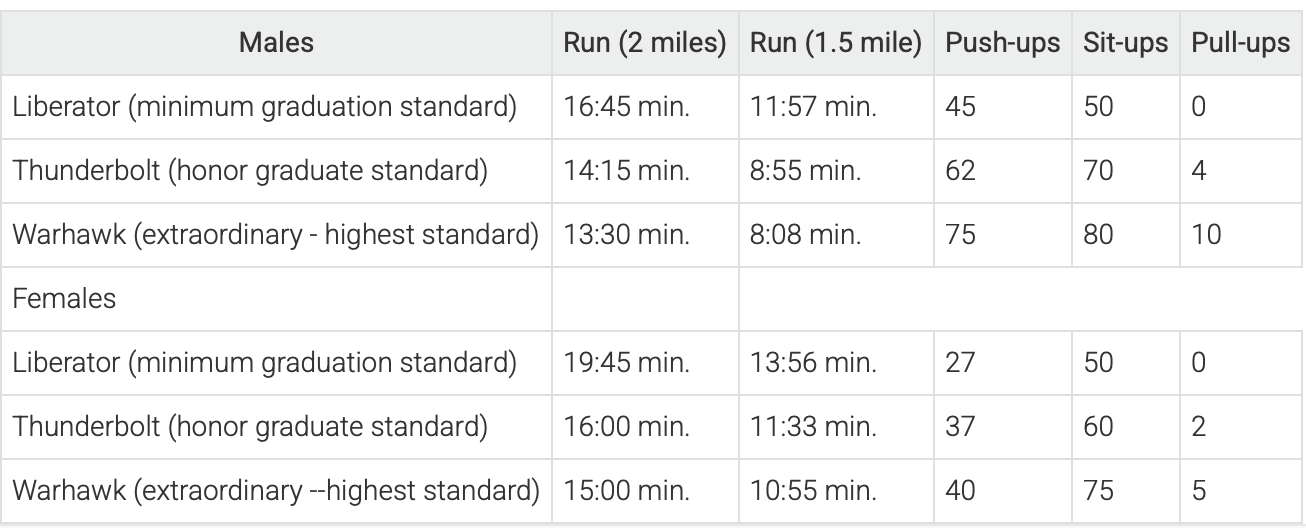
I think the US military’s standards do. They vary by branch and are changing, but here are some previous military fitness standards from the Air Force:
Pushups and sit-ups arehow many can be done in one minute
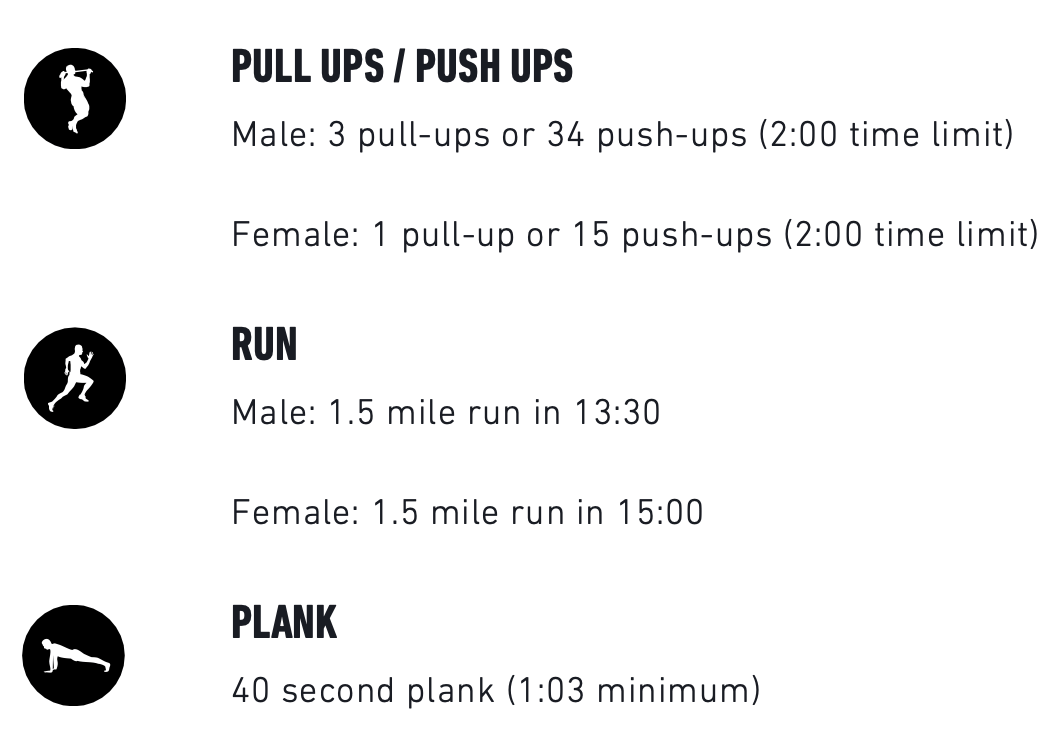
Here’s what the Marines expect from recruits before they show up for training:
The Army has a complex points system that varies by age and gender, but their minimum standards for a 20-year-old Male include: hex bar deadlift 150 lbs for 3 reps, 15 hand-release pushups within 2 minutes, plank for a minute 30, and a 2 mile run in 19:57 (plus their own sprint/drag/carry test in 2:28).
I like that the standards all involve a mix of strength and speed, and that they might take some work but should be achievable in a reasonable amount of time for a healthy person. I also like that they give stretch goals for the over-achievers in addition to their minimums.
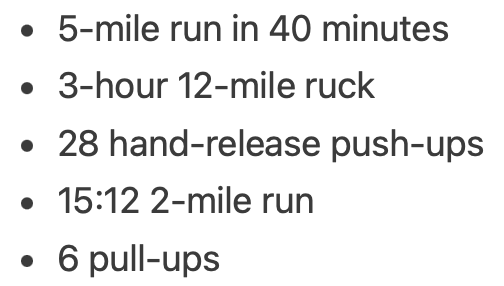
What about the real over-achievers, the ones who want to be not just “in shape” but “in great shape” or “in excellent shape”? For them, there are the special forces fitness tests. Here’s the Green Berets:
I’m in no way an authority on any of this, but for what it’s worth, you have my permission to say you’re in shape if you can meet any branch’s minimum requirements.
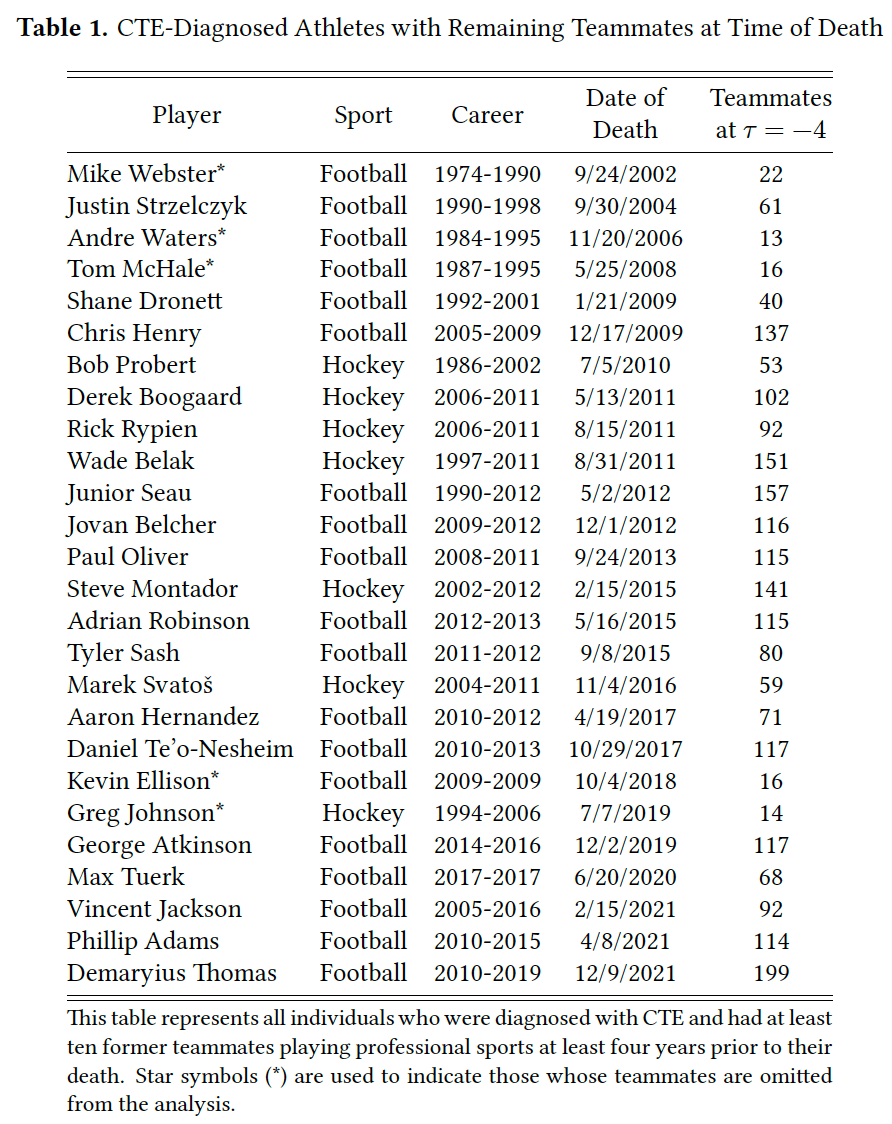
Formerteammates of athletes who died of CTE would require $6 million to offset this disamenity and $1million to be indifferent between exiting and staying in the profession.
So concludes a paper by Josh Martin. I thought this paper would be about a small group, since CTE deaths mostly happen among long-retired players with few or no former teammates still playing. But it turns out there were a fair number of early deaths, and each player had many teammates who can be affected, totaling 23% of NHL players and 14% of NFL players:
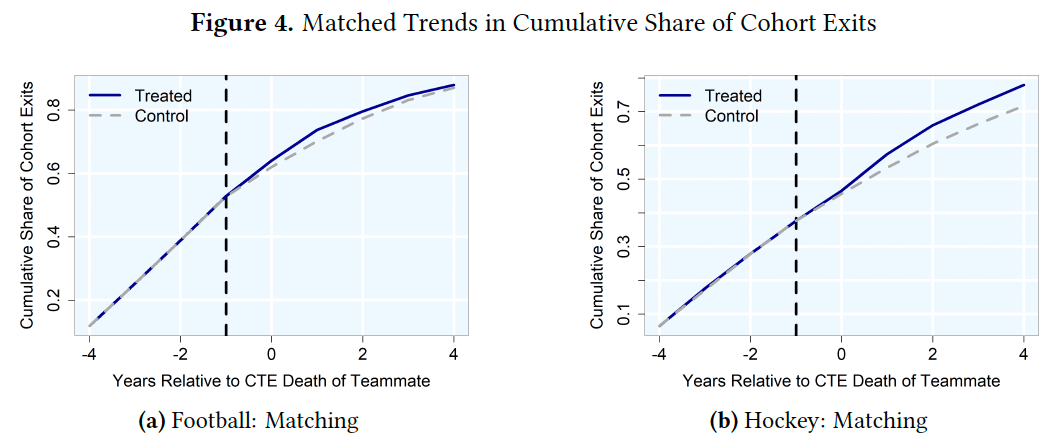
But teams mostly won’t pay worried players enough extra to stay, especially in hockey. So many of them retire early:
Athletes who were teammateswith a former teammate who died with CTE for three or more years and played for a team withthem at least two years before their death are 7.22 percentage points more likely to retire thancharacteristically similar non-treated players in the same years. Relative to the pre-treatmentmean, this represents a 69% increase.
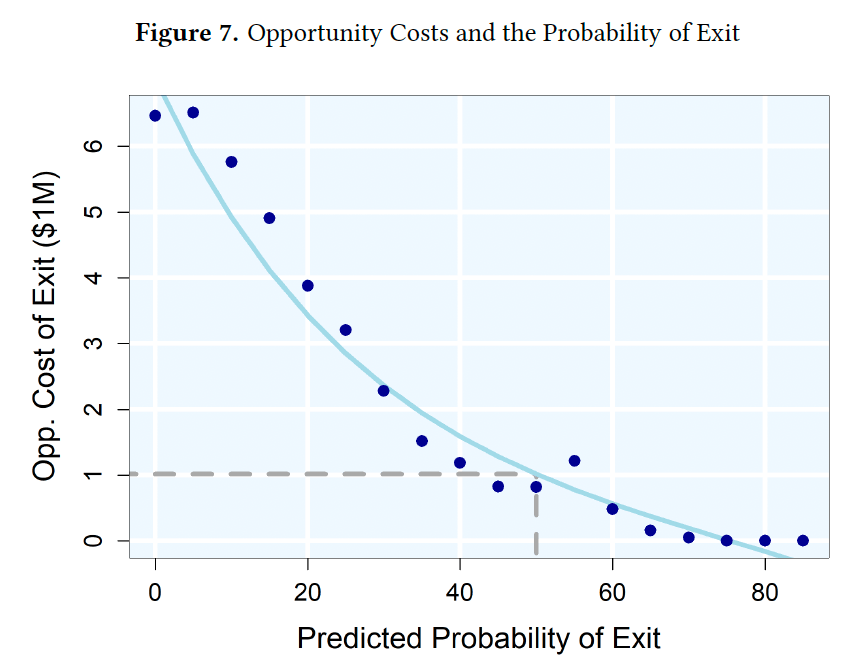
People still respond to incentives though, and if you do pay them enough they mostly take the risk and stay:
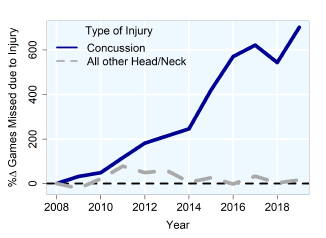
The remaining players will take measures to protect themselves, like skipping games to recover from concussions:
Michael previously pointed out here that these concerns matter more for certain positions, like running backs:
If you want millionaires to show up every week to willingly endure the equivalent of a half-dozen car accidents, you’re going to have to pay them.
This all makes for a good illustration of the theory of compensating differentials, which is sometimes surprisingly hard to observe in the labor market. But sports tend to have the sort of data we can only dream of elsewhere. Which other workers have millions of people observing, measuring, and debating their on-the-job productivity and performance?
This summer I was one of thousands of people crowding into Foxborough just to watch them practice:
The NFL season kicks off today, and I say the players deserve the millions they are about to earn.
The Affordable Care Act was supposed to make it easier for American workers to switch jobs by making it easier to get health insurance from sources other than their current employer. Mostly it didn’t work out that way. But a new paper finds that one piece of the ACA actually made people less likely to switch jobs.
The ACA Dependent Coverage Mandate required family health insurance plans to cover young adults though age 26, when prior to the 2010 passage of the ACA many had to leave the family plan at age 18 or 19. I thought these newly covered young adults would be more likely to switch jobs or start businesses, but there turned out to be absolutely no effect on job switching, and no overall increase in businesses (though it did seem to increase the number of disabled young adults starting businesses, and other parts of the ACA increased business formation among older adults).
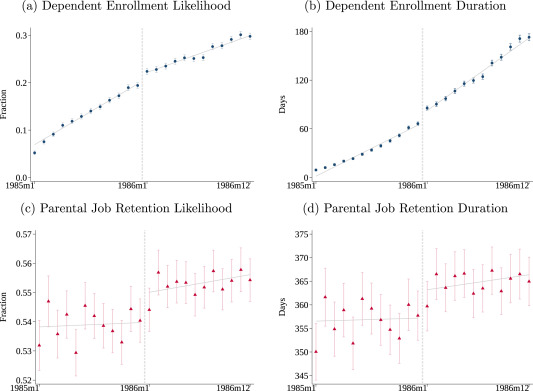
But while the Dependent Coverage mandate seems not to have reduced job lock for young adults, it increased job lock among their parents. That is the finding of a new paper in the Journal of Public Economics by Hannah Bae, Katherine Mackel, and Maggie Shi. Using a large dataset with exact months of age and coverage, MarketScan, allows them to estimate precise effects:
We find that dependents just to the right of the December 1985/January 1986 cutoff—those eligible for longer coverage—are more likely to enroll and remain covered for longer once the mandate is in effect. Dependent enrollment increases by 1.8 percentage points at the cutoff, an increase of 9.2 % over the enrollment rate for dependents born in December 1985. In addition, the enrollment duration increases by 9.7 days (14.6 %). Turning to their parents, we find that parental job retention likelihood increases by 1.0 percentage point (1.8 %) and job duration increases by 5.8 days (1.6 %) to the right of the cutoff. When scaled by the estimated share of dependents on end of year plans, our findings imply that 12 additional months of dependent coverage correspond to a 7.7 % increase in job retention likelihood and a 7.0 % increase in retention duration.
I believe in this parental job lock effect partly because of their data and econometric analysis, and partly through introspection. I plan to work for years after I have the money to retire myself in order to keep benefits for my kids, though personally I’m more interested in tuition remission than health insurance.
On top of working longer though, benefits like these enable employers to pay parents lower money wages. A 2022 Labour Economics paper from Seonghoon Kim and Kanghyock Koh found that the Dependent Coverage Mandate “reduced parents’ annual wages by about $2600 without significant reductions in the probability of employment and working hours.” But at least their kids are better off for it.
Iowa recently joined the growing list of states where midwives or obstetricians can open a freestanding birth center without needing to convince a state board that it is economically necessary. The Des Moines Register provides an excellent summary:
A Des Moines midwife who sued the state for permission to open a new birthing center may have lost a battle in court, but ultimately, she has won the war.
Caitlin Hainley of the Des Moines Midwife Collective sought to open a standalone birthing center in Des Moines, essentially a single-family home repurposed with birthing tubs and other equipment needed to give birth in a comfortable, home-like environment.
To do so, the collective alleged in its 2023 lawsuit, would have required going through a lengthy, expensive regulatory process that would give already established maternity facilities, such as local hospitals, the chance to argue against granting what is known as a certificate of need for the new facility, essentially vetoing competition.
A federal district judge ruled in November that Iowa’s certificate-of-need law is constitutional, finding that legislators had a rational interest in protecting existing hospitals and health care providers.
But while losing the first round in court, the collective’s cause was winning support in a more important venue: the Iowa Capitol. Iowa legislators in their 2025 session passed a bill, which Gov. Kim Reynolds signed on May 1, removing birth centers from the definition of health facilities covered by the certificate-of-need law. The law will formally take effect July 1.
I’m honored to have played a small part in this as the expert witness in the lawsuit.
If you’d like to get involved in making sure birth options are available your state, a great place to start would be to attend the Zoom seminar Roadmap For Reform: Advancing Birth Freedom on July 23rd. It is hosted by the Pacific Legal Foundation, which represented the midwives pro-bono in the Iowa case.
There is strong momentum here with Connecticut, Kentucky, Michigan, Vermont, and West Virginia also recently repealing Certificate of Need requirements for birth centers, but a variety of other barriers remain. States often require freestanding birth centers to obtain a transfer agreement with a nearby hospital before opening to ensure that the hospital will take their emergency cases, even though hospitals are legally required to take all emergency cases. The problem is that hospitals provide both complementary services (emergency care) and substitute services (labor and delivery), and they often choose not to sign transfer agreements in order to prevent competition from a partial substitute. This whole area would benefit both from more academic study, as well as more investigation from antitrust enforcement.
But for today, congratulations to Caitlin Hainley and to Iowa on their victory.















{kind=link}